This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I advised that perhaps posterior leads would help to persuade the interventionalist, since the 2022 ACC recommendations include posterior STEMI as a formal STEMI equivalent, but only officially by 0.5 Angiogram reportedly showed acute thrombotic occlusion of the first obtuse marginal which was stented. mm STE in the posterior leads.
This was interpreted by the treating clinicians as not showing any evidence of ischemia. Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. He was intubated in the field and sedated upon arrival at the hospital. Two subsequent troponins were down trending.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The baseline ECG is basically normal with no ischemia. In my opinion, I think it looks more like subendocardial ischemia.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. Clin Cardiol 2022 4. But no ECG met STEMI criteria so the patient was referred to cardiology as Non-STEMI. Lupu et al.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? The last echocardiography 12 months ago showed HFmrEF.
The benefits of QFR guidance are supported in a recent study that showed that a QFR-guided strategy of lesion selection for PCI improved two-year clinical outcomes, including reduction in myocardial infraction and ischemia-driven revascularization, when compared with standard angiography guidance alone.2 Leon, Shubin Qiao, Gregg W.
The cath lab was activated, and then not cancelled, and the angiogram showed 99% TIMI 2 flow proximal LAD culprit lesion, stented in less than 90 minutes of arrival. Cath days later showed complete occlusion of the LAD, stented. Ultimately, cardiac cath was done in Case #2, with stenting of the "culprit" LAD lesion.
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. Ischemia can be disguised by a wide escape rhythm, which decreases the sensitivity of ECG.
Method Between June 2018 and December 2022, 62 patients with type A aortic dissection (TAAD) underwent reoperation after previous surgical treatment. Outcome In the EVAR group, 47 patients (95.92%) were successfully implanted with overlapping stents, and 2 patients died in the perioperative period.
The pain will resolve and you will think the ischemia is gone when it is only hidden ! Just before 10 AM, the patient received a stent to the culprit OM. Smith comment: this troponin alone should be enough data to activate the cath lab, regardless of the ECG. Peak troponin was 12 ng/mL. Before and after angiography is shown below.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Whether these EKGs show myocarditis, a normal variant, or something else, they are overall not typical of transmural ischemia of the anterior or high lateral walls. It was stented.
I do not think this ECG is by itself diagnostic of OMI (full thickness, subepicardial ischemia ), b ut comparison to a previous might reveal this ECG as diagnostic of OMI. Clin Cardiol 2022; [link] Labs included: hsTnI 156 ng/L, Hb 12 g/dL, WBC 12x10^9/L, Cr. A single DES stent was placed, and the patient did well post-procedure.
It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chest pain. 2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. But it is still STEMI negative.
Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED. Angiogram soon after (around 4 hrs after presentation) showed multi vessel CAD, with culprit lesion total occlusion of the first obtuse marginal branch (OM1), which was stented.
The ECG was incorrectly interpreted as no signs of ischemia. Artificial intelligence can be trained to recognize subtle OMI = My Comment by K EN G RAUER, MD ( 2/6 /2023 ): = The initial ECG in today's case was incorrectly interpreted as, "No signs of ischemia". No further ECG were ever recorded.
Compare to the anatomy after stenting: The lower of the 2 now easily seen branches is the circumflex, now with excellent flow. Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia). 2022 Mar-Apr;71:44-46. Epub 2022 Jan 31.
This is where careful discussion with the patient is required, and an explanation of the most recent literature suggests no reduction in future major heart events with stenting in most obstructive coronary artery disease 5. ( 2022 Sep 16;101(37):e30583. 5 ISCHEMIA Research Group. Medicine (Baltimore). N Engl J Med. Eur Heart J.
This middle aged male with h/o GERD but also h/o stents presented to the ED with chest pain. He had been at a clinic that day where he had complained of worsening GERD. An EKG was reco rded and interpreted as normal by the computer, the clinician, and by the overreading cardiologist.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, This alone could be due to LVH, but V4 could NOT be due to LVH.
This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent. EKG shown here: LAFB with no clear signs of OMI or ischemia.
Delayed angiogram found a 95% mid RCA occlusion that was stented. Ischemic ST-segment depression maximal in V1-V4 (versus V5-V6) of any amplitude is specific for Occlusion Myocardial Infarction (versus nonocclusive ischemia). JAHA 2022 Grosmaitre P et al. Eur Heart J 2017 Driver BE, Shroff GR, Smith SW.
The operator performed intravascular ultrasound and visualized acute plaque rupture with thrombus formation and placed a stent. There was reperfusion ischemia superimposed on benign T-wave inversion. He is very lucky that he spontaneously reperfused and was stented before he had the chance to re-occlude.
It is not clear by her note what she meant by this (whether or not she recognized this EKG as diagnostic of transmural ischemia, and if so, of what territory) but emergent reperfusion therapy was not pursued. The proximal and mid LAD stenoses were stented and the OM 2 was left alone. Subendocardial ischemia does not localize.
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. He had a 100% RCA occlusion which was stented.
There is low voltage in the precordium which always makes reading ischemia harder. In ACS, chest pain is the warning sign of ongoing ischemia. Smith : As Willy says, and as we've said many times before, morphine will resolve pain without resolving ischemia. ECG 1 What do you think? To me, this ECG is not diagnostic.
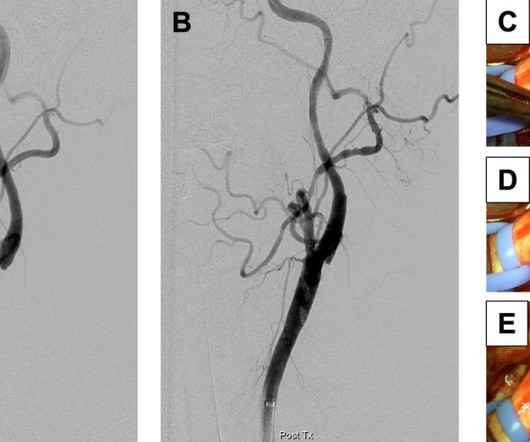
Management The web can create a flow disturbance, potentiating local thrombus formation, which can embolize producing resulting in cerebral ischemia. Current treatment is with anti-thrombotics and/or anticoagulation.Lesser option is to alter the flow disturbance caused by the web (surgery or stent). Ann Surg 1968; 167: pp.
He had undergone stenting of the LAD several weeks ago (unclear whether elective for stable symptoms, or in response to acute coronary syndrome). That the chief complaint of today's patient was acute CP ( C hest P ain ) with a history of known coronary disease and LAD stent placement a few weeks earlier. He appeared critically ill.
He eventually underwent CAG, where a circumflex occlusion was stented. This case highlights how T-waves are very important in the assessment of ischemia and dynamic changes in acute coronary syndrome. I have often seen colleagues worry about T-wave inversions as a sign of ongoing ischemia. Clin Cardiol [Internet].
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all. link] Bai, J., Tang, Z., &
The RCA was stented successfully with TIMI III flow noted post-procedure and the patient has done well with a post-PCI TTE demonstrating good LVEF and no wall motion abnormality. A good size infarct that no longer has active ischemia will have continually rising troponins due to the damage that was done hours ago.
It was opened and stented. Compared to TTE from 7/3/24: the anterior regional wall motion abnormality is new and is consistent with ischemia/infarction in the LAD territory == MY Comment , by K EN G RAUER, MD ( 11/20 /2024 ): == There are several insightful aspects of today's case. The October 21, 2022 post — for " artifactual VT".
Ischemia often produces a straightening of the ST segment and sometimes upward convexity. At cath later the same day, a proximal 99% RCA culprit lesion was stented. Discussion: When a patient presents with chest pain and ST segment elevation we need to evaluate whether or not the ST elevation is ischemic in nature.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content