This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
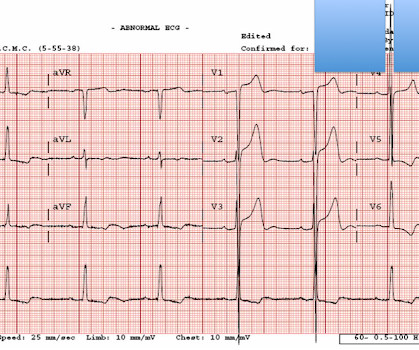
This confirms that the pain was ischemia and is now resovled. Review of the 2 ECGs in today's case is insightful ( Figure-1 ): The initial ECG shows sinus rhythm, LAHB and meets Peguero Criteria for LVH ( See My Comment in the August 15, 2022 post of Dr. Smith's ECG Blog for more on LVH criteria ).
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. Inferior hyperacute T waves, which have been added to the 2022 ACC consensus on chest pain as a “STEMI equivalent”[3] 3. J Am Coll Cardiol 2022 4. Curr Cardiol Red 2021 3. Kontos et al.
I advised that perhaps posterior leads would help to persuade the interventionalist, since the 2022 ACC recommendations include posterior STEMI as a formal STEMI equivalent, but only officially by 0.5 non-occlusive ischemia) Ongoing ischemic symptoms in NSTEMI is already an indication for emergent cath, regardless of the ECG.
High Diagnostic Accuracy Of AI-Ischemia in Comparison To PET, FFR-CT, SPECT, and Invasive FFR: A PACIFIC Sub-Study. Derivation, Validation and Prognostic Assessment of an AI-Based Algorithm for Determination of Coronary Ischemia: The CREDENCE and PACIFIC Trial. AJR Am J Roentgenol 2022 Sep;219(3):407-419. James Min, M.D.
In the October 15, 2022 post of Dr. Smith's ECG Blog — Drs. Smith and Meyers in their October 15, 2022 post on Precordial Swirl. Figure-3: Selected sets of V1,V2 leads from the examples of Precordial Swirl provided in the October 15, 2022 post in Dr. Smith's ECG Blog. What is P recordial S wirl ?
2022 Jul;27(4):e12939. Epub 2022 Feb 11. I last reviewed the phenomenon of electrical alternans in My Comment at the bottom of the page in the November 28, 2022 post of Dr. Smith's ECG Blog. Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia.
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy? How can you better assess the ST segments?
Osborn waves have been reported with hypercalcemia, brain injury, subarachnoid hemorrhage, Brugada syndrome, cardiac arrest from VFib — and — severe, acute ischemia resulting in acute MI ( See My Comment in the November 22, 2019 post on Dr. Smith’s Blog ). Rituparna et al — as well as Chauhan and Brahma ( Int.
In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. Remember that the RV is the most anterior chamber. Here is a transverse image of a CT showing this. A few clues that might have suggested this are: There is marked STE in V1.
In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) I interpret tracings systematically in "real time" ( including my assessment for acute ischemia ). The April 17, 2022 post ( Leads V1,V2 misplacement ). The May 5, 2022 post ( LA-RA reversal ).
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia. J Cardiol Cases.
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. This rules out subendocardial ischemia and is diagnostic of posterior OMI. The April 8, 2022 post by Drs.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Retrieved July 2, 2022, from [link] Moyé, D. Retrieved July 2, 2022, from [link] Sybrandy, K. Chest trauma was suspected on initial exam. Here is his initial ECG around 1330: What do you think? References Alborzi, Z.,
ACUTE MI (I allowed Acute MI to be in the report because I knew there would be an elevated troponin from ischemia, which is the definition of acute MI -- but in this case it would most likely be a Type 2 MI from tachycardia) There is also LA-RA lead reversal. The April 17, 2022 post ( Leads V1,V2 misplacement ).
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. Ischemia can be disguised by a wide escape rhythm, which decreases the sensitivity of ECG.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
There is probably a trickle of flow which is why there is both subendocardial ischemia (ST depression) and early subepicardial ischemia (hyperacute T-waves). And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! They are simply Hyperacute T-waves with depressed ST takeoff.
5] Back to the case The patient had serial ECGs over the next hour with no significant change: The first troponin came back at 1,400 ng/L (normal <26 in males and <16 in females), confirming MI – and the patient’s refractory ischemia indicated this was an Occlusion MI. Clin Cardiol 2022 4. Int J Cardiol 2024 3. Lupu et al.
A majority (62.5%) of those presenting with ‘normal’ ECGs had the cath lab activated without any ECG being labeled ‘STEMI’ by automated interpretation – based on signs of Occlusion MI including ECG changes, regional wall motion abnormality on bedside ultrasound, or refractory ischemia. 2022 ; 51 : 384 - 387 3. 2022 ; 55 : 180 - 182 6.
--The STD in V2-V6 might be interpreted as subendocardial ischemia, but with the inferior STE, it is far more likely to represent posterior OMI. In subendocardial ischemia, cath lab is indicated if the pain persists in spite of medical therapy (aspirin, anticoagulant, IV nitro). At 100 minutes, the above ECG was recorded.
As a result — IF no "fixable" cause is found ( ie, ischemia/infarction — electrolyte disturbance — rate-slowing medication ) — then because of the AV block and very slow heart rate, this patient will probably need a pacemaker. There are also twice as many P waves as QRS complexes — so at the least, there is 2nd-degree AV block.
My interpretation was: RBBB with hyperacute T-waves in V4-V6 that are all but diagnostic of LAD occlusion vs. post ROSC ischemia. As I emphasized in My Comment at the bottom of the page in the October 10, 2022 post in Dr. Smith's ECG Blog — Interpretation of a post-resuscitation ECG can be extremely challenging.
But ECGs interpretation is often conflated with clinical assessment, so if patients don’t present with chest pain the ischemic changes are not seen or are attributed to something other than ischemia. Problem #1: As I emphasized in My Comment in the December 6, 2022 post — Not all patients with acute MI report chest pain.
The pain will resolve and you will think the ischemia is gone when it is only hidden ! African Flag Sign provided by Dr. McLaren — with additional detailed discussion of this entity in My Comment at the bottom of the page in the May 11, 2022 post in Dr. Smith's ECG Blog ). Shmueli, H., Borohovitz, A., Matetzky, S., Gabarin, M.,
The differential is: Posterolateral OMI or subendocardial ischemia The distinction between posterior OMI and subendocardial ischemia can be important and sometimes difficult. Ischemic ST depression includes posterior OMI and subendocardial ischemia. Her prior ECG on file is shown below: What are your next steps?
Does this mean that the ST depression in V3 represents "anterior" subendocardial ischemia, and not posterior OMI? This is most consistent with ischemia/infarction in the distribution of the left circumflex coronary artery. non-occlusive ischemia) 2. Thus, they have much less voltage. They have ZERO ST Elevation.
This can be simply a equivalent of HT, with no true supply side ischemia with LVF with global ST depression ) Management *More or less similar to STEMI with aggressive opening of culprit lesions with few differences. 2022 Jun 20;11(12):3558. SCAI 2022 consensus update. Reference 1.Martínez J Clin Med. doi: 10.3390/jcm11123558.
I do not think this ECG is by itself diagnostic of OMI (full thickness, subepicardial ischemia ), b ut comparison to a previous might reveal this ECG as diagnostic of OMI. Clin Cardiol 2022; [link] Labs included: hsTnI 156 ng/L, Hb 12 g/dL, WBC 12x10^9/L, Cr. Unfortunately, they follow their own guidelines only 6% of the time!!
The ST/T wave ratio ( ie, the ratio of ST elevation compared to T wave amplitude ) in lead V6 is well over 0.24 ( See My Comment in the June 8, 2022 post for more on this Ratio ). That said — I did not interpret these differences as the result of acute ischemia. Spodick sign is present.
Data from 29 stroke centers for 10,229 AIS patients treated with MT for LVO between January 2010 and December 2022 was investigated. The primary outcome measure was successful recanalization defined as modified Thrombolysis in Cerebral Ischemia (mTICI) score of 2b or higher.
He got an MR, however that showed no scar or evidence of AVRD and he had a stress test with no evidence of inducible ischemia with almost 20 METs." He underwent an EP study 5/10/2022 for evaluation of pre-excitation/accessory tract which found a left sided accessory pathway - he is currently in the EP study now.
American Journal of Emergency Medicine 2022 4. Available from: [link] == MY Comment by K EN G RAUER, MD ( 4/22/2022 ): == It’s always difficult to try to “reconstruct events” when one wasn’t there. Was this objective evidence of inducible ischemia accompanied by chest pain? Bracey A, Meyers HP, Smith SW. Am J Med 2021 5.
We developed an ED triage diagnostic algorithm termed, “Dizzy-7”, based on evidence incorporating key history and physical examination elements derived in patients with acute posterior circulation ischemia. Stroke code activation occurred in nearly one in four (366/1599) these presentations.
Meyers — this initial tracing is diagnostic of acute LAD OMI with the precordial "Swirl" pattern ( I summarize "My Take" on recognizing Precordial "Swirl" at the bottom of the page in the October 15, 2022 post). Patients with precordial " Swirl " — have evidence of acute LAD OMI.
The anti-angiogenic impact of neutrophil elastase clouded the understanding of the role of neutrophils in promoting neovascularization (NV) and fibrinolysis in patients with chronic limb-threatening ischemia (CLTI). 2022 May;16(5):496-510. No hemorrhage occurred over the 30 day course. J Tissue Eng Regen Med. doi: 10.1002/term.3284
2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. The absence of STE in V7-V9 is often due to resolution of ischemia, as seen by resolution of ST depression in V7-V9. non-occlusive ischemia) JAHA 2021 3. -- Meyers HP, Bracey A, Lee D, et al.
Because previous ischemia induces myocardial preconditioning, decreasing the likelihood of transmural myocardial necrosis and myocardial rupture, patients with evidence of diabetes mellitus, chronic angina or previous MI are less likely to experience a rupture.
It is due to transmural ischemia not only of the anterior wall and apex, but due to transmural ischemia of the septum, usually due to occlusion proximal to the first septal perforator. Is this Acute Ischemia? The voltage is high but not huge. Read the case. More on LVH. This is LVH only, not OMI. This is LVH Only, not OMI.
Neurologic history is significant for right upper extremity weakness from 9/2022‐12/2022 that self‐resolved and was believed to be a peripheral nerve pathology. Admission exam without focal deficits. Admission CT of his head showed multifocal confluent hypodensities in the subcortical right frontal lobe.
Methods:236 AIS patients with low ASPECTS caused by LVO who undertook MT between January 2010 and December 2022 were retrospectively investigated. Univariate and multivariate logistic regression results were used to screen model predictors and construct nomograms of 90-day modified Rankin Scale scores (mRS) 0-3. with a score of 2, 17.7%
In this study, we aim to investigate the relationship between the number of MT passes at which successful recanalization is obtained and outcomes in LVO-related AIS patients with low ASPECTS.Methods:This retrospective cohort study was performed on the data from 31 thrombectomy-capable centers between 2013 to 2022.
It should be treated as such unless there is more information such as old or serial EKGs that can confirm a benign diagnosis, as BTWI patterns can mimic the South Africa Flag Sign (Compare this EKG to case 4 here: [link] com/2022/05/quiz-post-which- of-these-if-any-are-omi.html ). The patient had none of these conditions.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















































Let's personalize your content