This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
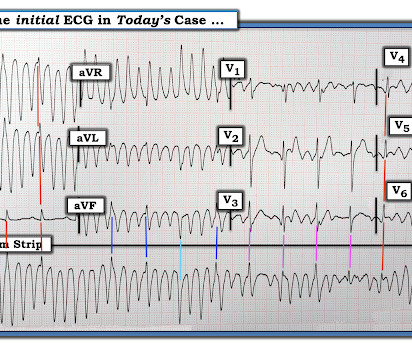
She was successfully revived after several rounds of ACLS including defibrillation and amiodarone. An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). 2022 Jul;27(4):e12939. Epub 2022 Feb 11. No ischemic ST changes. She was given magnesium empirically.
Artifact can obscure the rhythm or cause misdiagnosis of rhythms such as atrial fibrillation, ventricular tachycardia, and ventricular fibrillation. As worrisome as the initial recording in leads I and II look — a glance at lead III should immediately reassure us that defibrillation is not needed!
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. The April 8, 2022 post by Drs. This prompted cath lab activation. There is profound ST depression maximal in V1-V4.
From afar, there is gross tachycardia, cadence irregularities, and narrow QRS complexes that may, or may not, be Sinus in origin; and finally – a cacophony of wide complexes that might very well be ventricular in origin. McLaren : We’ve answered the first question – Sinus Tachycardia with episodic runs of wide QRS (RBBB morphology) and PVC’s.
IMPRESSION: Given the presence of a wide tachycardia — with 2 distinct QRS morphologies, and no sign of P waves — a presumed diagnosis of B i D irectional Ventricular Tachycardia has to be made. As reviewed by Almarzuqi et al ( Vasc Health Risk Mgmt 18:397-406, 2022 ) — Potential Causes of Bidirectional VT include: Digitalis toxicity.
There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). This episode self terminated before defibrillation was possible. This run of TdP is initiated by a PVC — but it then self-terminates. Discussion : The patient in today’s case presented with "seizures".
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). He required multiple defibrillations within a period of a few hours. An ICD ( Implantable Cardioverter Defibrilator ) was placed prior to discharge. What do you think?
The team immediately paged cardiology, concerned for polymorphic ventricular tachycardia. Since sinus conducted QRS complexes cannot co-exist together with ventricular tachycardia, this must all be artifact. The October 21, 2022 post — for " artifactual VT". The rhythm terminated before it could be captured on 12-lead.
It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. If you use quantitative end-tidal CO2 monitoring, there is never any need to waste time making sure that the endotracheal tube is correctly placed. == MY Comment, by K EN G RAUER, MD ( 10/10/2022 ): == Today’s case is a “Save”!
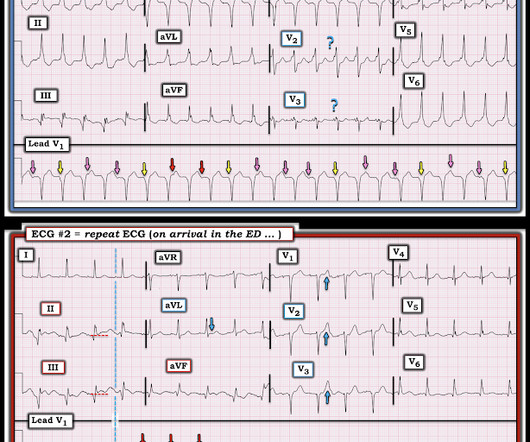
We can see enough to make out that the rhythm is sinus tachycardia. Tachycardia is unusual for OMI, unless the patient is in cardiogenic shock (or getting close). A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW.
This proves AV dissociation, and by extension ventricular tachycardia. The note lists a diagnosis of "tachycardia," which is described as "narrow complex." (The Repeat ECG obtained in ER: Fortunately for the patient, his ventricular tachycardia spontaneously resolved. Documentation lists a diagnosis of "sinus tachycardia."
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). This patient very likely has some form of idiopathic ventricular tachycardia. Of the ventricular outflow tract tachycardias (RVOT-VT) makes up 80-90%.
Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. She was defibrillated perhaps 25 times. Propranolol versus Metoprolol for treatment of electrical storm in patients with implantable cardioverter-defibrillator. SanzRuiz, R., Solis, J., &
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content