This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
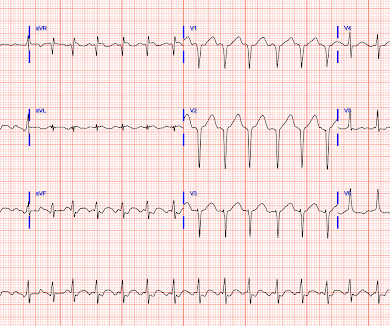
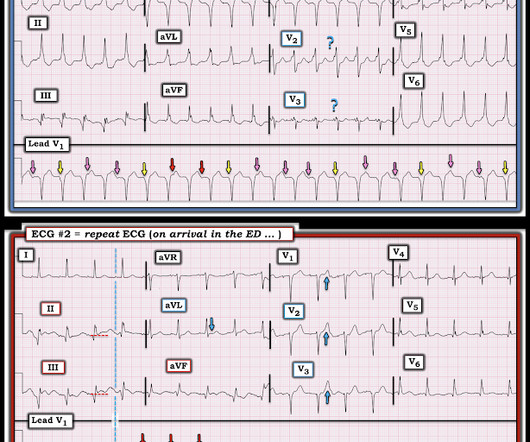
15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. Meyers and Smith in the October 15, 2022 post of Dr. Smith's ECG Blog ). 15, 2022 post — I like to focus on the ST-T wave appearance in leads V1 and V6 to facilitate recognition of Precordial Swirl. 15, 2022 post).
Introduction Wearable cardioverter-defibrillators (WCD) have emerged as a valuable tool in the management of patients at risk for life-threatening arrhythmias. These devices offer a non-invasive and temporary solution, providing continuous monitoring and the potential for prompt defibrillation when needed. years, with 78% being male.
ABSTRACT Background and Aims The safety and efficacy of the subcutaneous implantable cardioverter-defibrillator (S-ICD) has been proven in various clinical trials. Methods Between January 2018 and November 2022, a total of 99 consecutive patients underwent S-ICD device replacement. Data on device replacement strategies is scarce.
As reviewed by Almarzuqi et al ( Vasc Health Risk Mgmt 18:397-406, 2022 ) — Potential Causes of Bidirectional VT include: Digitalis toxicity. Despite prolonged resuscitation with multiple defibrillation attempts — the patient could not be saved. = CPVT ( Catecholaminergic PolyMorphic VT ). Acute myocardial ischemia.
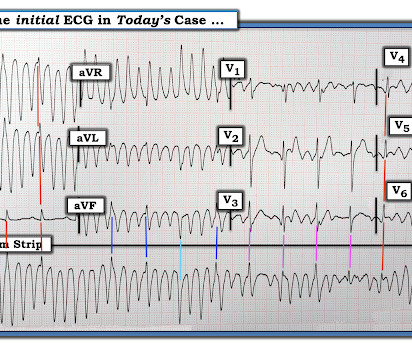
MY Thoughts on Today’s CASE: As tempting as it might be to reach for the defibrillator on seeing the ECG shown in Figure-1 — My initial reaction was different. The October 21, 2022 post — for " artifactual VT". What is the 1st thing — that YOU would do? Figure-1: I was sent this ECG without any history. Is this VT?
In November 2022, de-identified data from S-ICD devices in the LATITUDE monitoring system were analyzed. The research reported in this paper adhered to the Declaration of Helsinki (2013) and the Common Rule (45 CFR 46), ensuring that ethical standards were upheld despite the research involving de-identified data from human subjects.
Introduction Several studies have demonstrated that combining left ventricular ejection fraction and New York Heart Association functional class is insufficient for predicting risk of appropriate implantable cardioverter-defibrillator (ICD) shock in primary prevention candidates.
He underwent further standard resuscitation EXCEPT that we applied the Inspiratory Threshold Device ( ResQPod ) AND applied Dual Sequential Defibrillation (this simply means we applied 2 sets of pads, had 2 defib machines, and defibrillated with both with only a fraction of one second separating each defibrillation.
She was successfully revived after several rounds of ACLS including defibrillation and amiodarone. 2022 Jul;27(4):e12939. Epub 2022 Feb 11. I last reviewed the phenomenon of electrical alternans in My Comment at the bottom of the page in the November 28, 2022 post of Dr. Smith's ECG Blog. Ann Noninvasive Electrocardiol.
As this case shows, electrical capture isn't always possible at lower currents, especially with pads placed in a standard anterolateral "defibrillation" position. The University of Maryland found that capture occurred in only 42-78% of patients, dependent on pad positioning (Moayedi et al, 2022).
Primary preventive therapies, such as implantable cardioverter defibrillators, are not personalized and not predictive. All included ACP patients were recruited in 2009 at Yonsei University Hospital and were followed up until 2022. Most of these devices do not deliver life-saving therapy during their lifetime. years), 11 patients died.
He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. Some episodes of PMVT would terminate spontaneously — but on many occasions, the PMVT degenerated to VFib, requiring defibrillation.
We hypothesized an interaction effect and conducted stratified analyses to investigate whether witnessed arrest is more important than bystander CPR.MethodsThis study enrolled patients with outofhospital cardiac arrest between January 2010 and December 2022 in 3 emergency medical service (systems in Taiwan).
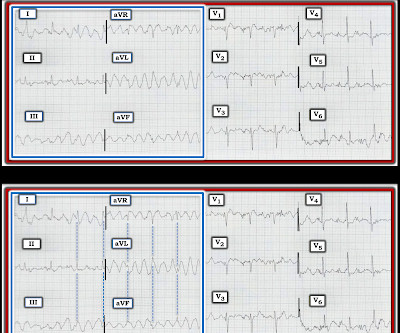
Searching for regular QRS complexes marching through potential artifact can help distinguish artifactual vs. actual ECG rhythms. == MY Comment, by K EN G RAUER, MD ( 10/19 /2022 ): == Today’s case by Dr. Meyers ( submitted by Dr. Arjun JV ) — is important for recognizing what it is not. This is not VFib or polymorphic VT!
003) and 2022 ESC risk model (log-likelihood ratios, -268.4 In the subgroup with Class 3 of recommendation for implantable cardioverter defibrillator, patients with absolute LV-GLS ≤ 9% showed significantly worse prognosis than those with absolute LV-GLS > 9% (p =.002 vs -266.2; vs -264.9; 009), respectively.
Tackling SCD was in God’s domain, until the brilliance of Dr. Michel Mirowski shrunk the defibrillator and implanted it under the chest in 1980. (Dr. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure.
Today's case reminds us of the intuitive logic that if a patient has a shockable arrest ( ie, VFib ) — and following successful defibrillation shows evidence of acute OMI ( even if STEMI criteria are not necessarily fulfilled ) — that such patients have much to gain from immediate cath with PCI. ( The April 8, 2022 post by Drs.
Methods Patients undergoing CIED surgery for approved indications between June 2015 and June 2022 were identified. The top two indications for the procedure included CIED generator change ( n = 9, 41%) and implantable cardioverter-defibrillator (ICD) implantation ( n = 7, 32%). The mean age was 50.2 ± 18.2
But artifact is "alive and well" — and learning to recognize it will amaze many of your colleagues ( and may serve to avoid an unnecessary defibrillation or two ). The October 21, 2022 post — for " artifactual VT". Like most clinicians — I learned about artifact "the hard way" = by seeing clinical cases that initially fooled me.
CASTLE-AF randomized 363 patients with atrial fibrillation and left ventricular ejection fraction of 35% or less, NYHA class II-IV heart failure and having an implanted defibrillator to either catheter ablation or medical therapy with rate or rhythm control [5]. 2022 Nov 22;146(21):1561-1563. Epub 2022 Nov 21. N Engl J Med.
Both the Comparison of Medical Therapy, Pacing and Defibrillation in Heart Failure (COMPANION) and the Cardiac Resynchronisation—Heart Failure (CARE-HF) trials [3,4], which were the cornerstone of electrotherapy in HF patients, showed up to a 36% reduction in mortality, an effect size rarely seen in trials today [5]. 2022, 9, 17.
This episode self terminated before defibrillation was possible. This run of TdP is initiated by a PVC — but it then self-terminates. ECG #3 Interpretation of ECG #3: This rhythm begins as Torsades de Pointes — that then becomes V-Fib. Discussion : The patient in today’s case presented with "seizures".
The patient was put on Extracorporeal Life Support in the ED 3 hours after initial resuscitation, the core temp was 30° C and the patient was defibrillated with a single attempt. On arrival, CPR was continued and core temperature was measured at 18° C (64.4° A 12-lead ECG was recorded: There is sinus rhythm with RBBB and right axis deviation.
We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG. Paradoxically, though, the third green arrow identifies a QRS that is more narrow than the RBBB complexes surrounding it. Question 2: What explains the conduction abnormalities? Indian Pacing and Electrophysiology Journal, 6(3), 182-83.
It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. If you use quantitative end-tidal CO2 monitoring, there is never any need to waste time making sure that the endotracheal tube is correctly placed. == MY Comment, by K EN G RAUER, MD ( 10/10/2022 ): == Today’s case is a “Save”!
Rhythm C: This telemetry strip from an older adult was initially thought to need defibrillation. The October 21, 2022 post — for " artifactual VT". Rhythm B: This patient was seen in the ED — and thought to be in AFlutter with 4:1 AV conduction. The March 17, 2023 post — for PTA. The January 17, 2023 post — for PTA.
When the ICD was finally interrogated, the syncopal events and shocks correlated with two VF events that were defibrillated successfully. The vessel was likely patent or nearly patent at the time of this ECG.
She was defibrillated and resuscitated. J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD.
We examined the effect of ibutilide, a class III antiarrhythmic agent, on the energy requirement for atrial defibrillation and assessed the value of this agent in facilitating cardioversion in patients with atrial fibrillation that is resistant to conventional transthoracic cardioversion. 25, 2022 ).
5] Immediate CPR and defibrillation are key to doubling the survival rate of cardiac arrest by 2030. 387 (2022): 1569-1578. In a 2023 consumer survey, over half of the participants said they would perform either CPR or Hands-Only CPR and that their confidence level in performing CPR has improved from 2021. [5] Circulation 147, no.
Methods Between September 2001 and June 2022, all consecutive patients with diagnosis of BrS were enrolled in the present study. Fifteen percent received appropriate implantable cardioverter-defibrillator (ICD) therapy and inappropriate ICD interventions were observed in 17%. 95% confidence interval: 0.7–19.6,
Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. She was defibrillated perhaps 25 times. Propranolol versus Metoprolol for treatment of electrical storm in patients with implantable cardioverter-defibrillator. SanzRuiz, R., Solis, J., &
The primary endpoint was survival at 180 days and freedom from implantable cardioverter-defibrillator (ICD), heart transplant/left ventricular assist device (LVAD), or readmission for heart failure. Between June 2022 and April 2024, 20 patients with CS (64 ± 8.9 years,
ABSTRACT Introduction The subcutaneous implantable cardioverter defibrillator (S-ICD) is an alternative to a transvenous ICD in patients who meet the criteria for ICD implantation without concurrent need for cardiac pacing. The objective of this study is to examine the rates of and indications for S-ICD removal and extraction.
In this case, you should get a second defibrillator and perform double sequential external defibrillation (DSED). Simply attach a second defibrillator as shown in the diagram below and deliver max shocks from both devices simultaneously. In the second case, the patient never converted meaning the shock did not do its job at all.
The submitter started the patient on amiodarone and arranged implantation of a defibrillator. == MY Comment , by K EN G RAUER, MD ( 12/27 /2024 ): == Superb discussion by Dr. Frick in today's case, that highlights a series of important points regarding the ECG recognition of stable VT ( V entricular T achycardia ).
Most patients can be managed without and implantable cardioverter defibrillator (ICD) In patients with PVCs/VT and a presentation not typical for an idiopathic origin cardiac magnetic resonance (CMR) should be considered, even if the Echo is normal. 2022, September 2) [2] Ward, R. Van Zyl, M., & & DeSimone, C. 3] Lavalle, C.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content