This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Post cath ECG: Now there are hyperacute T-waves again, and recurrent ST depression in V2 This ECG would normally diagnostic of OMI until proven otherwise No further troponins were measured, but it looks like there is recurrent OMI Next day: A CT CoronaryAngiogram was done (CTCA) CARDIAC MORPHOLOGY AND FUNCTION: 1. IMPRESSION: 1.
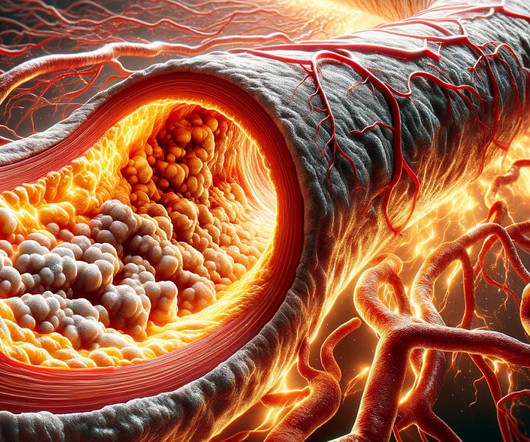
Reversing or regressing coronary artery disease is possible. You cannot eliminate the plaque entirely, but multiple clinical trials have shown plaque regression using high-intensity cholesterol-lowering treatments, which I have discussed previously. REVERSAL Investigators. 2004 Mar 3;291(9):1071-80.
A CT Coronaryangiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD LAD plaque with 0-25 percent stenosis. Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation."
The most accurate way (But not the only way) to answer this question is whether or not you have plaque in your coronary arteries. If you already have plaque, your risk of event an event goes up proportional to the amount of plaque you have 2. So, low risk by anyone’s books. Archives of Medical Science. 2022;18(6).
The coronaryangiogram revealed no critical stenosis, or acute plaque ulceration. Takotsubo should be a diagnosis of exclusion after angiography reveals no obstructive coronary disease, and repeat Echo displays left ventricular recovery. Furthermore, pertinent electrolyte values (e.g. Saini, A., Raymond-Paquin, A.,
We investigated the incidence of an acutely occluded coronary in patients presenting with STE-aVR with multi-lead ST depression. All electrocardiograms (ECGs) and coronaryangiograms were blindly analyzed by experienced cardiologists.
A CTCA provides much more anatomical detail and can identify advanced plaque often missed by CT Coronary Artery Calcium Score scans alone. CT Coronary Artery Calcium Score Scan CT Coronary Artery Calcium Score CT CoronaryAngiogram As you can see from the above images, the CTCA provides far more anatomical detail.
In these patients there is no plaque triggered ACS. we can witness menacingly deep resting ST depression with absolutely no thrombotic process going on in the coronary. Mind you, even a coronaryangiogram will not bail you out in terms of decision-making and risk prediction. 2022 Oct;38(10):1521-1524. Reference 1.
CT coronaryangiogram showed a hypoplastic RCA and dominant LCx. There were no plaques or stenoses. References: [1] 2022 ESC Guidelines for Ventricular Arrhythmias : Key Points - American College of Cardiology. 2022, September 2) [2] Ward, R. As noted above echocardiography was completely normal. Van Zyl, M., &
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content