This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The patient was a middle-aged female who had acute chestpain of approximately 6 hours duration. The pain was still active at the time of evaluation. Angiogram reportedly showed acute thrombotic occlusion of the first obtuse marginal which was stented. mm STE in the posterior leads. Peak troponin was not recorded.
No ChestPain, but somnolent. The fact that this is syncope makes give it a far lower pretest probability than chestpain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS. Former resident: "Just saw cath report, LAD stent was 100% acutely occluded."
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. He did not remember whether he had experienced any chestpain. (TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Two subsequent troponins were down trending.
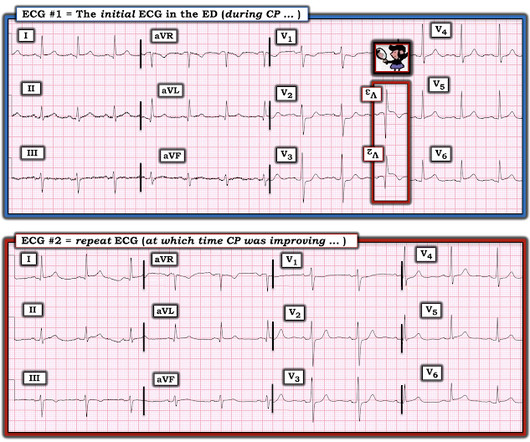
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). As a result, this 45-year old man did not experince any delay in treatment — and a large diagonal branch of the LAD was stented with good outcome.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? What do you think? This was the cost of preventing infarction of the anterior wall.)
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset. 2022 Jan;51:384-387.
Written by Jesse McLaren A previously healthy 50 year-old presented with 24 hours of intermittent exertional chestpain, radiating to the arms and associated with shortness of breath. In a previously healthy patient with new and ongoing chestpain, this is concerning for acute occlusion of the first diagonal artery.
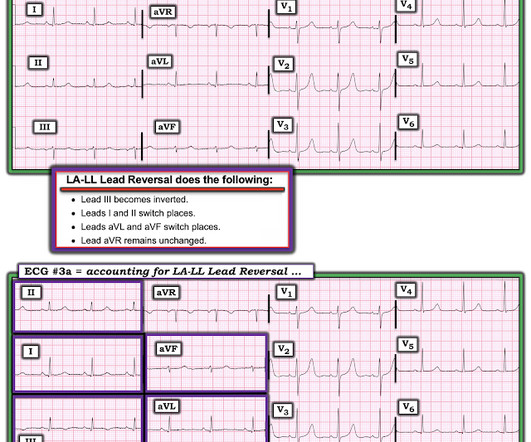
A 50-something man presented in shock with severe chestpain. Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. The April 17, 2022 post ( Leads V1,V2 misplacement ). The May 24, 2022 post ( LA-LL reversal ). The May 26, 2022 post ( LA-LL reversal ).
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. The Importance of the History: As noted above — the onset of chestpain in today's case was acute. He had received aspirin and nitroglycerin by EMS, with some improvement. His vitals were within normal limits.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. A single DES stent was placed, and the patient did well post-procedure.
A 50-something with no previous cardiac history and no risk factors presented to the ED with acute chestpain (pressure) that radiated to the left arm. It was stented with good results. An ECG was immediately recorded: Computer read: Normal ECG What do you think? There is ST depression in V1-V3.
Case submitted by Rachel Plate MD, written by Pendell Meyers A man in his 70s presented with chestpain which had started acutely at rest and has lasted for 2 hours. The pain was still ongoing at arrival. He also noted a bilateral "odd feeling" in his arms. He stated it was similar to prior heart attacks. Plate and Meyers.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, Pericarditis would be even more unlikely in someone without chestpain.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. Clin Cardiol 2022 4. The patient was transferred to CCU to consider surgical options. Lupu et al.
P.S.: Cardiac cath was performed — and showed a distal LA D "culprit" lesion that was successfully stented. The following are the KEY clinical and ECG features that establish the diagnosis of W ellens ' S yndrome : There should be a history of prior chestpain that has resolved at the time the defining ECG is obtained.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm).
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. It was stented. This was a large OMI.
See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. This is different from nitroglycerin which produces vasodilation and can improve by pain improving myocardial perfusion. Here is the angiogram after stent placement. See this case: A man his 50s with chestpain. At midnight.
The impact of this narrowing can ultimately result in angina (chestpain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardial infarction ( heart attack ) or even death. Leon, Shubin Qiao, Gregg W. If you enjoy this content, please share it with a colleague
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Published 2022 Feb 20.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chestpain. The first hs troponin I returned at 1100 ng/L Angiogram Lesion on 1st Obtuse Marginal : Proximal subsection = 90% stenosis Stented. He had no h/o heart failure. DBT was 120 minutes, pretty good for a Non-STEMI OMI.
He had concurrent sharp substernal chestpain that resolved, but palpitations continued. Over past 3 months, he has had similar intermittent episodes of sharp chestpain while running, but none at rest. Past medical history includes coronary stenting 17 years prior. IV Diltiazem was Contraindicated!
Sent by anonymous, written by Pendell Meyers Case 1: A man in his 50s presented with acute chestpain. The cath lab was activated, and then not cancelled, and the angiogram showed 99% TIMI 2 flow proximal LAD culprit lesion, stented in less than 90 minutes of arrival. Normal vital signs. Normal vitals. What do you think?
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chestpain that started within the last hour. The patient was found to have total "mid" LAD occlusion which was stented: Pre-PCI. The October 15, 2022 post in Dr. Smith's ECG Blog features no less than 20 ECG examples by Drs. What do you think?
He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. Successful primary angioplasty of the mid-circumflex artery towards the main marginal branch with the implantation of a drug-eluting stent. You must record frequent serial ECGs for patients with chestpain.
Written by Willy Frick A 40 year old woman was at home cooking when she developed chestpain. The operator documented thoughtful consideration of risks and benefits of stent placement. Technically, there was a very narrow landing zone for the stent, and missing this could result in "jailing" the LCx, which is ideally avoided.
This middle aged male with h/o GERD but also h/o stents presented to the ED with chestpain. The initial troponin I returned at 1500 ng/L and another ECG was recorded as the patient complained of 9/10 chestpain at 10 hours after the first Now the T-wave in III is fully upright, suggesting re-occlusion.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery. Regardless, if you present with chestpain and get a stress test instead of a CTCA, you are arguably getting an inferior test. I would say yes.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss. 2022 Mar-Apr;71:44-46.
Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED. Angiogram soon after (around 4 hrs after presentation) showed multi vessel CAD, with culprit lesion total occlusion of the first obtuse marginal branch (OM1), which was stented.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. She presented to the emergency department after a couple of days of chest discomfort. She also has a hx of paroxysmal atrial fibrillation and is on oral anticoagulant treatment. The last echocardiography 12 months ago showed HFmrEF.
Stent placed. Even if you don't see the OMI, you can usually prevent such a long delay to reperfusion by recording serial ECGs every 15 minutes for a patient with persistent chestpain. : Now it is not subtle: there is clear, obvious inferior posterior OMI. At this point, the cath lab was activated. Hillinger et al.
The lesion was successfully stented. The pain was completely resolved after coronary intervention. Comment by K EN G RAUER, MD ( 12/22 /2022 ): = Brilliant post by Dr. Aslanger — with emphatic illustration of "the difference in OMI vs STEMI philosophy" — in action! Aspirated thrombotic material. Turk Kardiyol Dern Ars.
Opened and stented. Here are over 30 cases of OMI which was interpretable on the ECG but which the computer called "normal." = Comment by K EN G RAUER, MD ( 12/23 /2022 ): = This is a “quickie case” that I like — because it reinforces a series of KEY principles essential to rapid decision-making.
A 40 something otherwise healthy man presented with substernal chestpain. They were stented. 2022 Jan;51:384-387. To amplify remarks by Dr. Smith above — considering the clinical context (ie, new-onset substernal chestpain ) — no less than 9/12 leads in ECG #1 are clearly abnormal. What do you think?
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
Case A 39-year-old male without prior medical history presents with chestpain that started 2 hours prior to presentation. He says that the pain intensity was 10/10 at home but now about 4/10. Despite the clinical stability and decreasing pain, this patient needs an immediate angiogram. 2022 Mar-Apr;71:44-46.
Delayed angiogram found a 95% mid RCA occlusion that was stented. JAHA 2022 Grosmaitre P et al. Available from: [link] == MY Comment, by K EN G RAUER, MD ( 2/10 /2022 ): == Superb post by Jesse McLaren — in which he traces the subtle but clearly-present evolution of acute Posterior OMI that was overlooked by health care providers.
Patient 2 : 55 year old with 5 hours of chestpain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. This was missed by the treating physician, but the chestpain resolved with aspirin. This was STEMI(-)OMI.
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. The patient has acute persistent refrectory chestpain and elevated troponin.
Written by Willy Frick A 51 year old man with hypertension presented with three hours of acute onset, severe midsternal chestpain associated with two episodes of nausea and vomiting. or 2) Inferior and lateral OMI that is beginning to reperfuse, even though the patient still has chestpain? ECG 1 What do you think?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content