This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
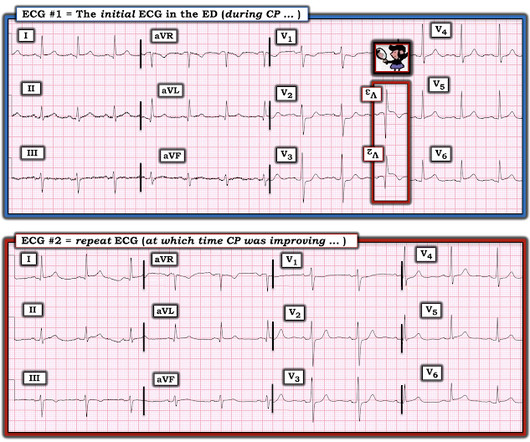
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
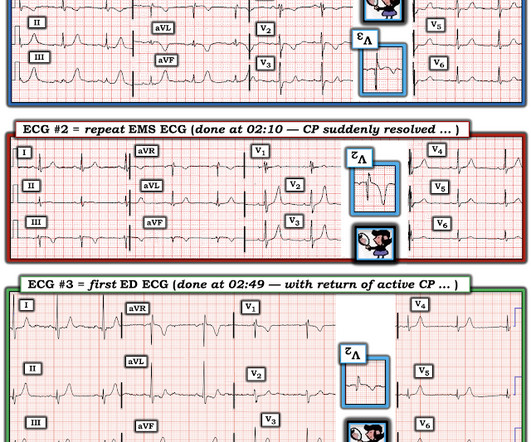
Sent by Drew Williams, written by Pendell Meyers A man in his 50s with history of hypertension was standing at the bus stop when he developed sudden onset severe pressure-like chestpain radiating to his neck and right arm, associated with dyspnea, diaphoresis, and presyncope. EMS arrived and administered aspirin and nitroglycerin.
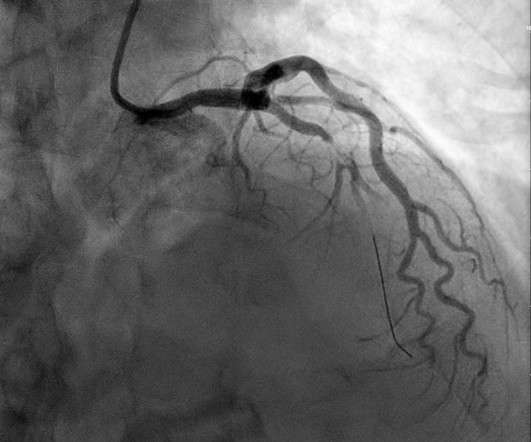
The ACC/AHA guidelines mandate less than 2 hours cath for patients with ACS with refractory pain, pulmonary edema, or electrical or hemodynamic instability. Angiogram at 4 hours after ECG 1 (and approximately 6 hours after pain onset): Culprit is 100% stenosis in the mid RCA. No wall motion abnormality.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Altogether, this strongly suggests inferolateral OMI, particularly in a patient with acute chestpain.
A 50-something with no previous cardiac history and no risk factors presented to the ED with acute chestpain (pressure) that radiated to the left arm. But even without these additional findings — the "Must Recognize" ECG pattern in this patient with new chestpain — is the unmistakeable shape of the ST depression in leads V2 and V3!
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin.
Upon questioning patient, he denies having any chestpain or chest tightness of any sort. In the absence of chestpain and negative troponin , it appears less likely that he is having acute coronary syndrome though EKG appears concerning. Pericarditis would be even more unlikely in someone without chestpain.
There is a patient with persistent chestpain and an initial troponin I over 52 ng/L; 52 ng/L has an approximate 70% PPV for acute type I MI in a chestpain patient. Clin Cardiol [Internet] 2022;Available from: [link] ECG 2: 35 minutes after arrival Ongoing OMI. Pain was severe and persistent.
Since the pathologist does not know the original cross-sectional area of the artery or the amount of compensatory enlargement of the artery from evaluation of a single cross section of the artery at a site of stenosis, the degree of luminal narrowing of that segment cannot be determined. These are typical findings at sites of plaque rupture.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm).
BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion).
Written by Pendell Meyers Both of these cases were sent to me with no information other than adults with acute chestpain. Case 1 An elderly male presented with chestpain. Case 2 A man in his 60s presented with acute chestpain, about 1 hour prior to evaluation: What do you think? We will study this soon.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Angiography revealed a 30% nonobstructive stenosis of the mid LAD.
Written by Pendell Meyers A man in his early sixties with no significant medical history (including a "negative cardiac workup a few years ago" for unclear indication) called 911 for acute chestpain constantly for the past 5 hours. However, this patient has active chestpain, and thus this this is inferior-posterior OMI.
Most cases go undiagnosed until the condition advances enough to create symptoms such as shortness of breath, chestpain or fatigue. Valvular heart disease, a condition in which any of the heart’s four valves are damaged or diseased, afflicts 2.5 percent of all Americans and 13 percent of Americans over age 80.
Method We discuss a unique case where a patient had headache attacks without chest symptoms, autonomic dysfunction, or triggers. We reviewed English case reports of cardiac cephalalgia from 1982 to 2022 using PubMed ([link] Results A 69-year-old man presented with a sudden headache without triggers or typical symptoms.
If you saw this ECG only knowing that it is an acute chestpain patient, what would be your interpretation? However, in the context of the first ECG and the waning chestpain, this is diagnostic of reperfusion. Due to the severity of the pain and the high BP, they obtained an aortic dissection CT.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chestpain. The first hs troponin I returned at 1100 ng/L Angiogram Lesion on 1st Obtuse Marginal : Proximal subsection = 90% stenosis Stented. He had no h/o heart failure. link] Case continued The cath lab was activated rapidly.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? Here is the clinical informaton on ECG 2: A man in his 50s presented to the Emergency Department with acute chestpain that started within the past few hours.
This middle aged male with h/o GERD but also h/o stents presented to the ED with chestpain. The initial troponin I returned at 1500 ng/L and another ECG was recorded as the patient complained of 9/10 chestpain at 10 hours after the first Now the T-wave in III is fully upright, suggesting re-occlusion.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Angiography : LMCA — 90-99% osteal stenosis. The below ECG was recorded.
Written by Pendell Meyers, edits by Smith Two patients presented with acute chestpain/pressure. Here is the South African Flag sign ( Figure by Ken Grauer — with the original 12-lead from Patient 1 attached below — See his Comment from the April 8, 2022 post in Dr. Smith's ECG Blog for more on this sign ).
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. Anything more on history? Left main?
Written by Willy Frick A 40 year old woman was at home cooking when she developed chestpain. The cardiologist called this 20% stenosis. Unfortunately, a few hours later the patient complained of recurrent chestpain. She took an oxycodone and called EMS. Her presenting ECG is shown below: ECG 1 What do you think?
There was no chestpain. I’ve reviewed My Take on the ECG diagnosis of RVH on a number of occasions in Dr. Smith’s ECG Blog ( See My Comment at the bottom of the page in the March 6, 2022 and September 1, 2020 posts , to name just 2 ). But today's patient had no chestpain. How Does this Apply to Today’s Case?
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
A 62 year old man with hyperlipidemia presented to a rural emergency department with 7 hours of 3/10 chestpain. In this case, it is possible that the physicians interpreted the ST depression in anterior leads as subendocardial ischemia of the anterior wall, and the mid LAD stenosis as the culprit of that ischemia.
This was submitted by a paramedic, Hailey Kennedy A late 50s male called 911 following 2 hours of chestpain that started while working at his desk. He reported the crushing chestpain radiated down his left arm. He presented to the ED for evaluation chestpain. Pain was improved but not gone upon arrival.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content