This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
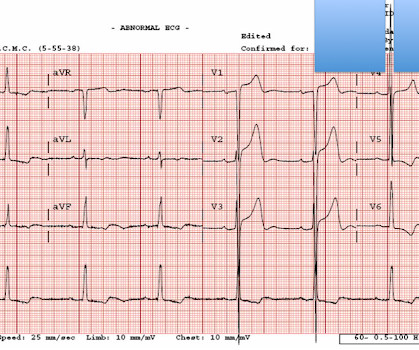
Written by Jesse McLaren, with a very few edits by Smith A 60-year-old presented with chestpain. The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. J Am Coll Cardiol 2022 4. But are there any other signs of Occlusion MI? Kontos et al.
The patient was a middle-aged female who had acute chestpain of approximately 6 hours duration. The pain was still active at the time of evaluation. non-occlusive ischemia) Ongoing ischemic symptoms in NSTEMI is already an indication for emergent cath, regardless of the ECG. mm STE in the posterior leads.
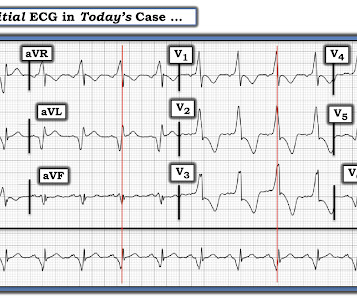
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). In any case, the ECG is diagnostic of severe ischemia and probably OMI. All ECGs were recorded by EMS, and transferred to a PCI capable center for evaluation.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible.
Written by Jesse McLaren Four patients presented with chestpain. Other signs of OMI that complement the ECG include new regional wall motion abnormalities and refractory ischemia References 1. 2022 ; 51 : 384 - 387 3. 2022 ; 55 : 180 - 182 6. Hughes KE , Lewis SM , Katz L , Jones J. Acad Emerg Med. Am J Emerg Med.
Another ECG was recorded after the nitroglycerine and now without pain: All findings are resolved. This confirms that the pain was ischemia and is now resovled. The history is concerning ( This patient was awakened from sleep by chestpain that persisted for several hours — on a background of intermittent CP in recent weeks ).
I went to the patient's chart: Elderly woman with stuttering chestpain and SOB, and dizziness. The unique " shape " of the prominent ST-T wave abnormalities in this tracing — that are much more suggestive of some significant form of LVH ( L eft V entricular H ypertophy ) rather than ischemia. What do you think now?
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Triage VS: 135/65 mmHg, 95 bpm, 94% on room air, 16/min, 98.6 Lupu L, et al.
--The STD in V2-V6 might be interpreted as subendocardial ischemia, but with the inferior STE, it is far more likely to represent posterior OMI. Here is the history: A 40-something male had intermittent chest discomfort until 90 minutes prior to presentation, when it became constant. At 100 minutes, the above ECG was recorded.
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. The ECG was incorrectly interpreted as no signs of ischemia. The Importance of the History: As noted above — the onset of chestpain in today's case was acute. His vitals were within normal limits.
Sent by Drew Williams, written by Pendell Meyers A man in his 50s with history of hypertension was standing at the bus stop when he developed sudden onset severe pressure-like chestpain radiating to his neck and right arm, associated with dyspnea, diaphoresis, and presyncope. Is this Acute Ischemia? More on LVH.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. American Journal of Emergency Medicine 2022 4.
Written by Jesse McLaren, with edits from Smith and Grauer A 60 year old with no past medical history presented with two hours of chestpain radiating to the left arm, with normal vitals. 2] Conduction through the accessory pathway can be intermittent (with different degrees of pre-excitation), and affected by ischemia.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin. J Am Heart Assoc.
Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS.
Submitted and written by Quinton Nannet, MD, peer reviewed by Meyers, Grauer, Smith A woman in her 70s recently diagnosed with COVID was brought in by EMS after she experienced acute onset sharp midsternal chestpain without radiation or dyspnea. Ischemic ST depression includes posterior OMI and subendocardial ischemia.
2 days later This is a typical LVH pattern, without ischemia Patient underwent 4 vessel CABG. Upon questioning patient, he denies having any chestpain or chest tightness of any sort. Pericarditis would be even more unlikely in someone without chestpain. Chestpain is squeezing or tight in nature.
These were texted to me only with "chestpain." It helps to know that the patient has active chestpain, as Wellen's is a post occlusion (reperfusion) state, with open artery and pain-free. And ECGs can change and evolve even when there is no ischemia. First: 2nd: What was my response? It was indeed.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
A 67 yo f developed chestpain this morning." There is probably a trickle of flow which is why there is both subendocardial ischemia (ST depression) and early subepicardial ischemia (hyperacute T-waves). And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!!
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. Clin Cardiol 2022 4. But no ECG met STEMI criteria so the patient was referred to cardiology as Non-STEMI.
NOTE: It's important to correlate ongoing circumstances at the time that a prior tracing was done ( ie, Was the patient stable and asymptomatic — or were they having chestpain, an exacerbation of heart failure, or some other ongoing process at the time the prior ECG was recorded? ). What is P recordial S wirl ?
Because previous ischemia induces myocardial preconditioning, decreasing the likelihood of transmural myocardial necrosis and myocardial rupture, patients with evidence of diabetes mellitus, chronic angina or previous MI are less likely to experience a rupture. Not all patients with acute ( or recent ) MI have chestpain with their event.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. For now she can only say Not OMI.
My interpretation was: RBBB with hyperacute T-waves in V4-V6 that are all but diagnostic of LAD occlusion vs. post ROSC ischemia. As I emphasized in My Comment at the bottom of the page in the October 10, 2022 post in Dr. Smith's ECG Blog — Interpretation of a post-resuscitation ECG can be extremely challenging.
Written by Willy Frick A 50 year old man with no medical history presented with acute onset substernal chestpain. In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. His ECG is shown below.
Context: a man in his 40s presented to the emergency department with 1 day of sudden onset chestpain. The ST/T wave ratio ( ie, the ratio of ST elevation compared to T wave amplitude ) in lead V6 is well over 0.24 ( See My Comment in the June 8, 2022 post for more on this Ratio ). Pericarditis maybe." Spodick sign is present.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. It is also important to recognize that BTWI patterns can be very dynamic.
It is due to transmural ischemia not only of the anterior wall and apex, but due to transmural ischemia of the septum, usually due to occlusion proximal to the first septal perforator. A 50-something with cocaine chestpain and ST Elevation in V1 - V3 This one is very tough. Is this Acute Ischemia? Read the case.
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy?
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma? Retrieved July 2, 2022, from [link] Moyé, D.
Sent by anonymous, written by Pendell Meyers Case 1: A man in his 50s presented with acute chestpain. Click here to sign up for Queen of Hearts Access Case 2: A woman in her 60s presented with acute chestpain. Normal vital signs. Here is his ECG at triage: What do you think? Normal vitals. What do you think?
A 40-something woman with diabetes and peripheral vascular disease who frequently needs the ED for chronic pain called 911 for sudden severe chestpain. Does this mean that the ST depression in V3 represents "anterior" subendocardial ischemia, and not posterior OMI? non-occlusive ischemia) 2.
A 40-something male with no previous cardiac disease presented with chestpain. Here is his ECG: There is no clear evidence of OMI or ischemia. This is suspicious for inferior reciprocal At this point, with continued pain, cath lab activation is indicated. even in the absence of ECG findings.
She was hemodynamically stable — and did not have chestpain, lightheadedness or syncope. As a result — IF no "fixable" cause is found ( ie, ischemia/infarction — electrolyte disturbance — rate-slowing medication ) — then because of the AV block and very slow heart rate, this patient will probably need a pacemaker.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? Here is the clinical informaton on ECG 2: A man in his 50s presented to the Emergency Department with acute chestpain that started within the past few hours.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. Anything more on history? J Electrocardiol 2013;46:240-8 2.
Superimposed OMI cannot be ruled out, but the patient has syncope, not chestpain. Here are many more examples of this: See this recent post: Chestpain and anterior ST depression. What’s the cause(s)? Would you have recognized the acute posterior OMI? How I wish we had follow-up on this case.
This is the prehospital ECG from an 81 year old man with acute chestpain. I favor the P s, Q s, 3 R Approach — as a simple acronym to facilitate recall of the 5 KEY Parameters for rhythm interpretation ( See My Comment in the October 25, 2022 post in Dr. Smith’s ECG Blog ). The medics did NOT activate the cath lab. Arrhythmia?
This middle aged male with h/o GERD but also h/o stents presented to the ED with chestpain. The initial troponin I returned at 1500 ng/L and another ECG was recorded as the patient complained of 9/10 chestpain at 10 hours after the first Now the T-wave in III is fully upright, suggesting re-occlusion.
The message is clear — If, in a patient with new chestpain — ST-T wave depression is maximal in leads V2 , V3 and/or V4 — consider acute posterior MI until proven otherwise. C ASE C onclusion : On their way to the hospital, the EMS crew requested cath lab activation — because they recognized the above "dynamic" ST-T wave changes.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
RVOT VT: A 40-something without past history presents with wide complex tachycardia and crushing chestpain Regular Wide Complex Tachycardia. He got an MR, however that showed no scar or evidence of AVRD and he had a stress test with no evidence of inducible ischemia with almost 20 METs." There is no inferior axis.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content