This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
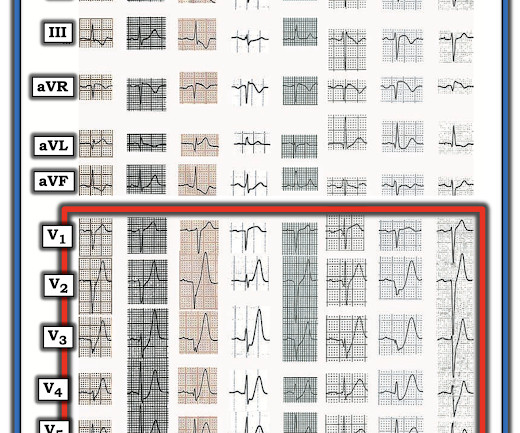
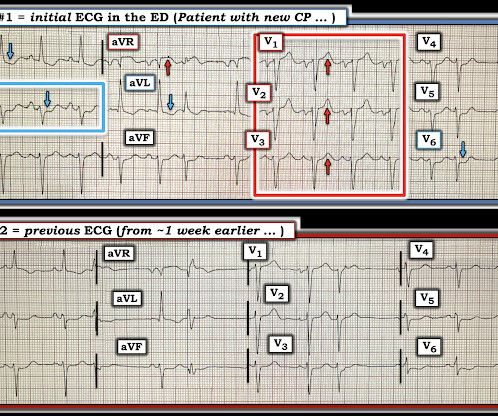
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Do either, both, or neither have occlusion MI? Vitals were normal.
A 50-something man presented in shock with severe chestpain. The patient was in clinical shock with a lactate of 8. The April 17, 2022 post ( Leads V1,V2 misplacement ). The May 24, 2022 post ( LA-LL reversal ). The May 26, 2022 post ( LA-LL reversal ). The August 17, 2022 post ( LA-RA reversal ).
The VSR is what is causing the cardiogenicshock! Mechanical complications occur acutely and significantly alter hemodynamics leading to comp ensatory mechanism which usually involve vasoconstriction and tachycardia, both hallmarks of cardiogenicshock. PIRP is strongly associated with myocardial rupture.
Case submitted by Rachel Plate MD, written by Pendell Meyers A man in his 70s presented with chestpain which had started acutely at rest and has lasted for 2 hours. The pain was still ongoing at arrival. He was in cardiogenicshock requiring an impella for several days after cath. Plate and Meyers.
Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenicshock). But the History in today's case was acute shortness of breath with dizziness and lightheadedness — and, essentially without chestpain! Additionally, there is borderline right axis deviation.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
This is one case where it made a difference: Right Ventricular MI seen on ECG helps Angiographer to find Culprit Lesion Nevertheless, it is sometimes a fun academic exercise to try to predict the infarct artery: An elderly patient had onset of chestpain one hour prior. His included cardiogenicshock, V Tach, AV block.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. An elderly man with sudden cardiogenicshock, diffuse ST depressions, and STE in aVR Literature 1.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Tachycardia is unusual for OMI, unless the patient is in cardiogenicshock (or getting close).
The following are the KEY clinical and ECG features that establish the diagnosis of W ellens ' S yndrome : There should be a history of prior chestpain that has resolved at the time the defining ECG is obtained. The ChestPain required for the definition of Wellens' Syndrome occurred at the time of coronary occlusion.
He had concurrent sharp substernal chestpain that resolved, but palpitations continued. Over past 3 months, he has had similar intermittent episodes of sharp chestpain while running, but none at rest. A 50-something presented with s udden onset palpitations 8 hrs prior while sitting at desk at work. Patient intubated.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm).
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
He stated later that he gave her 1 sublingual NTG and her pain went down to 1/10. Shes in impella dependent cardiogenicshock w new renal failure. This 60-year old woman clearly presented to the ED as a higher -risk patient given her history of known coronary disease, now with new chestpain. Post cath ekg here.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
Written by Willy Frick A woman in her 60s with very severe hyperlipidemia (LDL >200 mg/dL) presented with acute onset chestpain. She described the pain as moderate in severity, and said it had come and gone several times over the next few hours before ultimately resolving. Her symptoms began while getting off the bus.
Written by Pendell Meyers An adult man presented with acute chestpain. See our other cases with similar patters, to burn this deep into your brain files: Smith : In my experience, these cases of LAD OMI with RBBB and LAFB are either about to arrest, post-arrest, and/or in cardiogenicshock. He appeared critically ill.
Sent by anonymous, written by Pendell Meyers A woman in her 40s with no known comorbidities presented with acute chestpain radiating to left arm and neck, which started approximately 4 hours prior to arrival. What is the Diagnosis in this 70-something with ChestPain? 68 minutes with chest compressions, full recovery.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content