This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Pendell Meyers A man in his 50s was found by his family in cardiacarrest of unknown duration. Despite anticipation by many that the initial post-resuscitation ECG will show an obvious acute infarction — this expected "STEMI picture" is often not seen. 15, 2022 post). As per My Comment in the above-cited Oct.
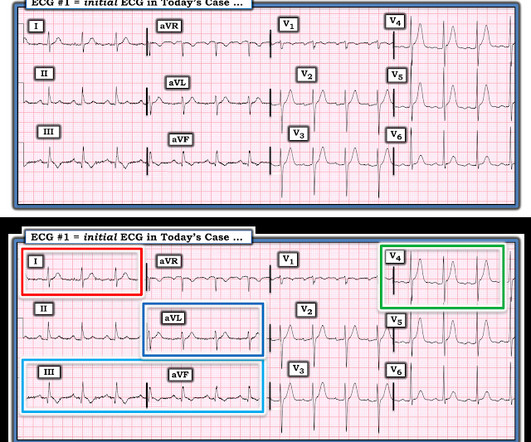
Shortly after arrival in the ED ( E mergency D epartment ) — she suffered a cardiacarrest. BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Figure-1: The initial ECG in today's case — obtained after successful resuscitation from cardiacarrest. ( No CP ( C hest P ain ).
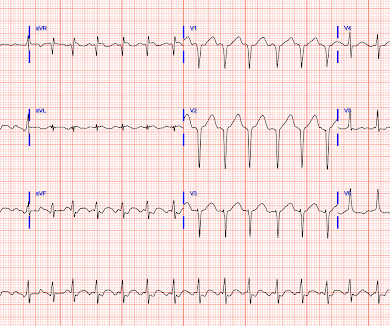
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI. The April 8, 2022 post by Drs.
Subtle as a STEMI." (i.e., About 45 minutes after the second EKG, the patient was found in cardiacarrest. Later the next day, she went into cardiacarrest again. By the time I saw the repeat EKG, the patient was already in cardiacarrest. None of the 20 ever evolved to STEMI criteria.
He had multiple cardiacarrests with ROSC regained each time. Then there is loss of pulses with continued narrow complex on the monitor ("PEA arrest") Learning Points: Sudden witnessed CardiacArrest due to ACS is almost always due to dysrhythmia. This patient arrested shortly after hospital arrival.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. First — Some thoughts on the post -resuscitation ECG.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Figure-1: The initial ECG in today’s case.
Past medical history included RBBB without other cardiac history, but old ECG was not available. The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
She was diagnosed with a Non-STEMI and kept overnight for a next day angiogram. Medics recorded the above ECG and called a STEMI alert. The patient went into arrest pre-hospital. Her symptoms at the time ECG #1 was obtained were CP and SOB — yet interpretation of this initial tracing prompted a STEMI alert.
About an hour later, he was then found on the floor in cardiacarrest in the ED. Sooner identification likely leads to better outcomes, and in this case may have allowed prevention of cardiacarrest and better long-term outcome. His initial troponin T was 15 ng/L (only two hours since pain onset). Plate and Meyers.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. Meyers and Smith illustrate 20 example cases vs "look-alikes" of Swirl ( with my synthesis of "Swirl" ECG findings in My Comment on that post ) from October 15, 2022. The below ECG was recorded.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
For technical reasons — P waves are not well visible in this tracing — BUT — the P wave in lead I appears to be larger than the P wave in lead II , which is often a tip-off to LA-LL Reversal ( See My Comment in the November 19, 2020 and the May 24, 2022 posts in Dr. Smith's ECG Blog ).
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". Hyperkalemia mimics STEMI and OMI in many distributions, but probably the most common is the Brugada morphology in V1-V2 which mimics anterior OMI for those who cannot recognize the Brugada pattern. HyperKalemia with CardiacArrest.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. BOTTOM Line: It can at times be extremely challenging to distinguish between anterior ST elevation from a benign Brugada Phenocopy pattern vs an acute anteroseptal STEMI.
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. She was defibrillated and resuscitated.
See many examples of Pseudo STEMI due to hyperkalemia at these two posts: Acute respiratory distress: Correct interpretation of the initial and serial ECG findings, with aggressive management, might have saved his life. No followup EKG was recorded!! Figure-1: Reasons for the difficulty determining the rhythm with severe hyperkalemia.
There is worrisome T-wave inversion in inferior leads as well, which is another clue to LAD Occlusion In fact, this ECG meets STEMI criteria!! Why does the conventional algorithm not diagnose STEMI? Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04 All intervals and the axis are normal.
ECG met STEMI criteria and was labeled STEMI by computer interpretation. J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). Take home : Not all STEs are STEMIs or OMIs. What do you think?
Acute chest pain, right bundle branch block, no STEMI criteria, and negative initial troponin. Plus recommendations from a 5-member panel on cardiacarrest. Plus recommendations from a 5-member panel on cardiacarrest. These are often VERY difficult to recognized. Protocols can be overridden by Physician Judgment.
Unexplained cardiacarrest or documented VF/polymorphic VT: +3 3. Unexplained sudden cardiac death (3 categories) (+0.5 - +2) 4. Cardiacarrest. Clinical History 2.a. of atrial fib/flutter at age less than 30: +0.5 syncope of unclear etiology: +1 2.c. Suspected arrhythmic syncope: +2 2.d. Family History 3.a.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content