This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
No ChestPain, but somnolent. The fact that this is syncope makes give it a far lower pretest probability than chestpain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS. Here is the ED ECG (a photo of the paper printout) What do you think?
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? That is, until the 7th R wave which comes a little bit sooner than expected. What do you think?
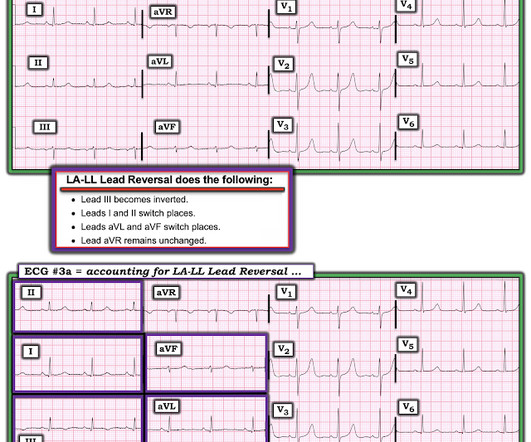
A 50-something man presented in shock with severe chestpain. Here is his ED ECG: There is bradycardia with a junctional escape. Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. The April 17, 2022 post ( Leads V1,V2 misplacement ). The May 24, 2022 post ( LA-LL reversal ).
Case An 82 year old man with a history of hypertension presented to the ED with chestpain at 1211. He described his chestpain as pleuritic and reported that it started the day prior while swinging a golf club. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin.
The rhythm is sinus bradycardia at a rate just over 50/minute. Although difficult to measure ( because of marked overlap of the QRS in multiple chest leads ) — there appears to be greatly increased QRS amplitude, consistent with voltage for LVH. The April 17, 2022 post ( Leads V1,V2 misplacement ).
Written by Jesse McLaren, with edits from Smith and Grauer A 60 year old with no past medical history presented with two hours of chestpain radiating to the left arm, with normal vitals. Unfortunately, the reality is — that many ( most ) WPW patients who present with chestpain do not manifest intermittent preexcitation.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
She was hemodynamically stable — and did not have chestpain, lightheadedness or syncope. Even if we stopped here — We could conclude the following: There is marked bradycardia in today's rhythm ( ie, Heart rate in the low 30s ). QUESTIONS: HOW would you interpret the rhythm in Figure-1 ? Is this " high -grade" AV block?
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. It is also important to recognize that BTWI patterns can be very dynamic.
This middle aged male with h/o GERD but also h/o stents presented to the ED with chestpain. The computer called "Sinus Bradycardia" only (implying that everything else is normal. The overreading Cardiologist called it only "Sinus Bradycardia" with no other findings. There is zero ST Elevation.
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chestpain: V5 and V6 sure look like a STEMI For this ECG and chestpain in the ED, the Cath lab activated. But the angiogram was clean.
A 40-something male with no previous cardiac disease presented with chestpain. The pain continued and the first high sensitivity troponin I returned at 105 ng/L Another ECG was recorded: The ST segment in aVF has flattened a bit, revealing that there is some STD in addition to the non-specific findings in III and aVL.
Even if you don't see the OMI, you can usually prevent such a long delay to reperfusion by recording serial ECGs every 15 minutes for a patient with persistent chestpain. The rhythm in ECG #1 is sinus bradycardia and arrhythmia. Did YOU notice that leads V1 and V2 of ECG #4 were placed too high on the chest?
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. What do you think?
After the heart rate increased slightly, here was the repeat ECG: Sinus bradycardia, only slightly faster rate than prior. See these similar cases: A man in his sixties with chestpain Why is there inferior ST elevation, and would you get posterior leads? Sudden CP and SOB with Inferior ST Elevation and in STE in V1.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
She did notice something slightly wrong subjectively, but had no palpitations, chestpain, or SOB, or any other symptom. Baseline bradycardia in endurance athletes limits the use of ß-blockers. 25, 2022 ). This middle-aged patient has a remote history of cardiac surgery as a young child for a "heart murmur".
Written by Jesse McLaren A 75 year old with a history of CABG called EMS after 24 hours of chestpain. There’s sinus bradycardia, normal conduction, normal axis, delayed R wave progression, and normal voltages. Sinus bradycardia.” paramedic transportation to the ED as “chestpain, STEMI negative” 2.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
His first electrocardiogram ( ECG) is given below: --Sinus bradycardia. Comment by K EN G RAUER, MD ( 12/22 /2022 ): = Brilliant post by Dr. Aslanger — with emphatic illustration of "the difference in OMI vs STEMI philosophy" — in action! As he seemed very agitated, fentanyl and diazepam were given. Turk Kardiyol Dern Ars. 2021.21026.
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. He complained of generalized weakness and left lower extremity numbness. What is it? Activate the Cath Lab?
Although in the context of chestpain such ST depression would be all but diagnostic of posterior OMI, one should make no conclusions in such an unusual case. In all leads, there is a 2nd wave after the initial QRS. This is an Osborn wave. I have not found any previous report of Osborn waves in RBBB.
Patient 2 : 55 year old with 5 hours of chestpain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. This was missed by the treating physician, but the chestpain resolved with aspirin.
Despite the baseline artifact theres sinus bradycardia, convex ST elevation in III, reciprocal ST depression in aVL and possible anterior ST depression indicating inferoposterior OMI. He was given two separate sprays of nitroglycerin sublingually, neither of which improved his pain but did cause him to become briefly hypotensive ( 600 ng/L.
He then provided some history: " Classic story for angina, few hours of crushing chestpain." The rhythm is sinus bradycardia at ~55-60/minute. The Mirror Test in lead V3 is clearly positive ( See My Comment at the bottom of the page in the September 21, 2022 post). What are the ECG Findings?
days of chestpain that started as substernal and crushing in nature awakening him from sleep and occasionally traveling to right side of neck. The pain was described as constant, worse with deep inspiration and physical activity, sometimes sharp. He reported 1.5
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. He told the patient this horrible news. link] Bai, J., Tang, Z., & Verbeek, P.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content