This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Methods Consecutive patients with bradycardia indicated for pacing from 2016 to 2022 were prospectively followed for the clinical endpoints of heart failure (HF)-hospitalizations and all-cause mortality at 2 years. CSP should be preferred over VSP or RVP during pacing for bradycardia.
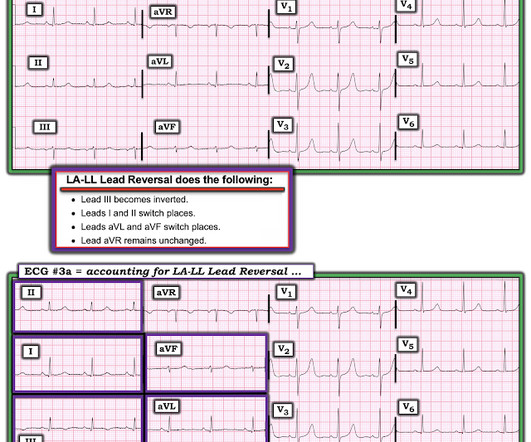
The rhythm is sinus bradycardia at a rate just over 50/minute. The April 17, 2022 post ( Leads V1,V2 misplacement ). The May 5, 2022 post ( LA-RA reversal ). The May 24, 2022 post ( LA-LL reversal ). The May 26, 2022 post ( LA-LL reversal ). The August 17, 2022 post ( LA-RA reversal ).
Background Rotational atherectomy (RA) during percutaneous coronary intervention may cause transient bradycardia or a higher-degree heart block. Traditionally, some operators use prophylactic transvenous pacing wire (TPW) to avoid haemodynamic complications associated with bradycardia. No patients underwent prophylactic TPW insertion.
Altered Mental Status, Bradycardia == MY Comment , by K EN G RAUER, MD ( 2/2 /2024 ): == Dr. Meyers began today’s case with the clinical challenge of asking you to identify the underlying cause of ECG #2. -- Read this ECG -- Osborn Waves and Hypothermia (this is the "Figure" above) What does LBBB look like in severe hypothermia?
A recently opened clinical trial called BACKBEAT (BradycArdia paCemaKer for Blood prEssure treAtmenT) aims to use Medtronic’s Astra and Azure model pacemakers to not only treat slow heart rates but also delivers electrical pulses stimulating the heart in a way that reduces the patient’s blood pressure.
Even if we stopped here — We could conclude the following: There is marked bradycardia in today's rhythm ( ie, Heart rate in the low 30s ). Finally — If today's patient does not have significant underlying coronary disease — then her bradycardia with AV block may be the result of SSS ( S ick S inus S yndrome ).
Retrieved July 2, 2022, from [link] Moyé, D. Retrieved July 2, 2022, from [link] Sybrandy, K. Retrieved July 2, 2022, from [link] == MY Comment , by K EN G RAUER, MD ( 2/4 /2024 ): == Today's case by Dr. The ST-T wave in leads V5,V6 looks to be disproportionately large ( ie, hyperacute ) given QRS amplitude in these leads.
Consecutive patients who underwent LBBP in our team from June 2022 to November 2022 were enrolled. This study aims to compare the clinical outcomes between transthoracic echocardiography (TTE)- and X-ray-guided LBBP. Methods This is a single-center, prospective, randomized controlled study.
Other cardiac-related causes for syncope associated with acute MI may include malignant ventricular arrhythmias and bradyarrhythmias including AV block.
I will leave more detailed rhythm discussion to the illustrious Dr. Ken Grauer below, but this use of calipers shows that the rhythm interpretation is: Sinus bradycardia with a competing (most likely junctional) rhythm. preceding each of the fascicular beats — indicating a faster rate for the escape rhythm compared to the sinus bradycardia ).
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. Limiting one's interpretation to marked bradycardia with high-grade AV block in need of pacing in this patient with multiple syncopal epiosodes — more than suffices for "the quick answer".
There was no evidence bradycardia leading up to the runs of PMVT ( as tends to occur with Torsades ). If there had been — a temporary atrial pacemaker could have been considered as a way of increasing the heart rate to suppress a bradycardia-dependent arrhythmia ("overdrive pacing").
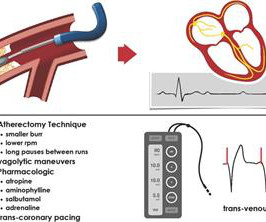
Learning points: TCP is primarily recommended for bradycardia that does not respond to atropine, or other agents. The University of Maryland found that capture occurred in only 42-78% of patients, dependent on pad positioning (Moayedi et al, 2022). The patient was ultimately discharged with a poor neurologic outcome.
formed a strategic collaboration for the development and commercialization of AVIM therapy for hypertensive pacemaker patients in July 2022. Our collaboration with Orchestra BioMed will explore how cardiac pacing can go beyond management of bradycardia and conduction disease to treat hypertension as well,” said Robert C. Kowal, M.D.,
Here is his ED ECG: There is bradycardia with a junctional escape. Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. The April 17, 2022 post ( Leads V1,V2 misplacement ). The May 24, 2022 post ( LA-LL reversal ). The May 26, 2022 post ( LA-LL reversal ).
The purpose of this case series is to provide an overview of the procedural and clinical outcomes of patients who underwent stenting for symptomatic ICAS.MethodsWe reviewed a database of all interventional procedures conducted at our institution to identify patients who underwent intracranial stenting from 2013 and 2022 for symptomatic ICAS.
Hyperkalemia causes peaked T waves and the "killer B's of hyperkalemia", including bradycardia, broad QRS complexes, blocks of the AV node and bundle branches, Brugada morphology, and otherwise bizarre morphology including sine wave. With a twist. Do you recognize this ECG yet? Right Bundle Branch Block with ST Elevation in V1?
Re ECG recognition of SA Block — See My Comment at the bottom of the page in the May 25, 2022 post — as well as my comment in the Addendum of the August 30, 2023 post.
It should be treated as such unless there is more information such as old or serial EKGs that can confirm a benign diagnosis, as BTWI patterns can mimic the South Africa Flag Sign (Compare this EKG to case 4 here: [link] com/2022/05/quiz-post-which- of-these-if-any-are-omi.html ). Patient 1 remained in the hospital overnight.
The computer called "Sinus Bradycardia" only (implying that everything else is normal. The overreading Cardiologist called it only "Sinus Bradycardia" with no other findings. The rhythm in Figure-1 is sinus bradycardia and arrhythmia. Here is the old ECG from 6 years prior: Notice the inferior T-waves have normal size here.
As a reminder of why determination of the cardiac rhythm can be so challenging when there is significant hyperkalemia — I've reproduced Figure-1 from My Comment in the January 16, 2022 post in Dr. Smith's ECG Blog. Figure-1: Reasons for the difficulty determining the rhythm with severe hyperkalemia. WHY Isn't the QRS Wide?
Three months prior to this presentation, he received a pacemaker for severe bradycardia and syncope due to sinus node dysfunction. A troponin T was drawn at 1229 and resulted slightly elevated at 23 ng/L (URL for men in this assay is 15 ng/L). The ED provider ordered a coronary CT scan to assess the patient for CAD.
After the heart rate increased slightly, here was the repeat ECG: Sinus bradycardia, only slightly faster rate than prior. For readers not familiar with this format — I've reviewed its features in the Addendum at the bottom of the page in the April 24, 2022 post in Dr. Smith's ECG Blog.
L/min, BP 107/65 mm Hg, HR 71 bpm LVEF 45%, no wall motion abnormality The patient had a complete neurologic recovery, proving once again that the patient is not dead until he/she is warm and dead. == MY Comment by K EN G RAUER, MD ( 2/8/2022 ): == I thought this to be an intriguing case for a number of reasons.
Blunt Trauma in a Child 40-something male in a head-on Motor Vehicle Collision and Splenic Injury == MY Comment, by K EN G RAUER, MD ( 10/10 /2022 ): == Highly interesting post by Dr. Smith regarding a 30-something male with multiple injuries from a motor vehicle accident. What are the ECG Findings of Cardiac Contusion?
The rhythm in ECG #1 is sinus bradycardia and arrhythmia. Increased J-point ST depression, with downslope sagging ST segments and terminal T wave positivity ( ie, markedly positive "Mirror" Test — as per My Comment in the September 21, 2022 post of Dr. Smith's ECG Blog ) — confirms acute posterior OMI.
This is guideline approved by both ACC/AHA and by European guidelines. == Comment by K EN G RAUER, MD ( 6/1/2022 ): == I found serial evaluation of sequential tracings in today's case to be subtle — yet highly insightful. A patient with active chest pain and an otherwise unexplained elevated troponin should go to the cath lab.
His first electrocardiogram ( ECG) is given below: --Sinus bradycardia. Comment by K EN G RAUER, MD ( 12/22 /2022 ): = Brilliant post by Dr. Aslanger — with emphatic illustration of "the difference in OMI vs STEMI philosophy" — in action! As he seemed very agitated, fentanyl and diazepam were given. Turk Kardiyol Dern Ars. 2021.21026.
Triage physician interpretation: -sinus bradycardia -lateral ST depressions While there are lateral ST depressions (V5, V6) the deepest ST depressions are in V4. The screening physician ordered an EKG and noted his ashen appearance and moderate distress. Triage EKG: What do you think?
Int J Cardiol 2014. == MY Comment by K EN G RAUER, MD ( 10/13/2022 ): == I suspect most cases of acute OMI that occur in association with WPW — are overlooked! Wolff-Parkinson-White syndrome ‘cured’ by myocardial infarction? CMAJ 2014. Chang and Liu. Wolf-Parkinson-White syndrome influenced by myocardial infarction.
Baseline bradycardia in endurance athletes limits the use of ß-blockers. 25, 2022 ). Clinically — The importance of factoring in increased vagal tone as a contributing factor to AFib episodes — extends into management. Vagally-mediated AFib is more likely to occur at night or after meals — and less likely to occur with exercise.
Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. CJEM 2021 == MY Comment, by K EN G RAUER, MD ( 1/3/2022 ): == Excellent case presentation by Dr. Jesse McLaren! What do you think? There’s primary ST depression in the precordial leads maximal in V3-4, and an inverted T wave in V2.
There’s sinus bradycardia, normal conduction, normal axis, delayed R wave progression, and normal voltages. The patient has a history of CABG so some of these changes could be old, but with ongoing chest pain and bradycardia in a high risk patient this is still acute OMI until proven otherwise. Sinus bradycardia.” Kontos et al.
Patient 2 : 55 year old with 5 hours of chest pain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. Smith : The fact that the ECG did not evolve is further proof that this was the baseline ECG. nearly identical to the first case).
This ECG shows a sinus bradycardia with a normal conduction pattern (normal PR, normal QRS, and normal QTc), normal axis, normal R-wave progression, normal voltages. Hypothermia can also produce bradycardia and J waves, with a pseudo-STEMI pattern. Can J Cardiol 2022 Kukla P, Jastrezebski M, Praefort W. What do you think?
I've listed potential causes of acute pericarditis in My Comment at the bottom of the page in the June 11, 2022 post in Dr. Smith's ECG Blog. Pediatric cardiology performed a bedside echo in ED with EF estimation of 60%, no pericardial effusion, and no regional wall motion abnormalities.
Methods A retrospective analysis of all patients who underwent S-ICD implantation between 2010 and 2022 at a single multihospital healthcare system was performed. years was 5.9%, with the most common indications for extraction being the need for bradycardia pacing, infection, and inappropriate shocks due to oversensing.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. After this ECG was obtained, the ER physician received word that the patient's husband had died in the crash. He told the patient this horrible news. link] Bai, J., Tang, Z., & Verbeek, P.
Despite the baseline artifact theres sinus bradycardia, convex ST elevation in III, reciprocal ST depression in aVL and possible anterior ST depression indicating inferoposterior OMI. Still, an ECG was obtained at 0649hrs: (Digitized by PM Cardio) McLaren: The patient has a high pretest probability based on age, risk factors and symptoms.
MY Thoughts on ECG #1: The rhythm is sinus bradycardia at a rate just under 60/minute. Figure-1: The initial ECG in today's case — obtained from a woman with CP. ( To improve visualization — I've digitized the original ECG using PMcardio ). Intervals ( PR, QRS, QTc ) and the axis are normal. No chamber enlargement.
There are 2 main options: Overdrive pacing could be considered and in the right clinical situation, this is often effective for reducing ventricular arrhythmias ( especially in the case of preventing pause induced or bradycardia-induced arrhythmias in association with QTc prolongation ). 2022, September 2) [2] Ward, R. Van Zyl, M., &
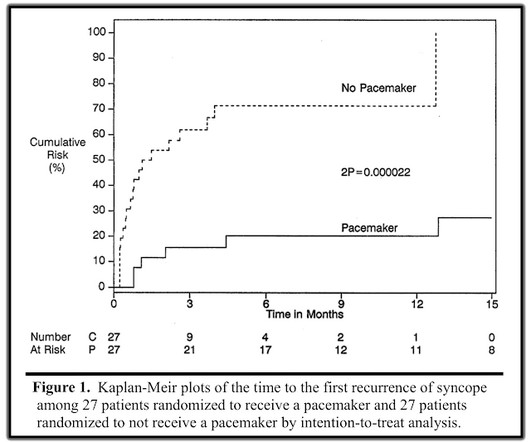
Perhaps because the bradycardia in vasovagal syncope is only one part of the autonomic response. Phase 4 block is also referred to as "bradycardia dependent block." A stunning result. One of many examples in medical history that remind us of the importance of blinding in clinical trials. Why was there no benefit?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content