This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
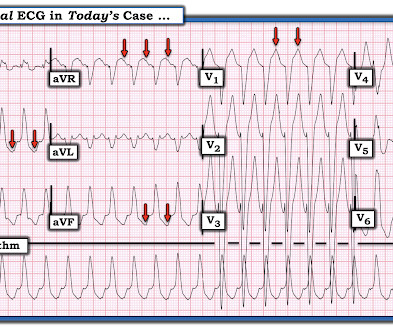
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
She also has a hx of paroxysmal atrialfibrillation and is on oral anticoagulant treatment. She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Cardiac output (CO) was being maintained by the tachycardia.
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation. What to do?
Introduction A high recurrence rate of atrialfibrillation was monitored after catheter ablation for persistent atrialfibrillation. Trial Registration Registered with Chinese Clinical Trials Registry on 27 August 2022, identifier: ChiCTR2200062995.
Backgroundwide antral pulmonary vein isolation (PVI) is effective for treating paroxysmal atrialfibrillation (PAF), although time-demanding. Procedural data and electrophysiology (EP) laboratory times were systematically collected and analyzed.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Atrialfibrillation is also a predictor of worse outcomes in this case (Alborzi). Retrieved July 2, 2022, from [link] Moyé, D. Retrieved July 2, 2022, from [link] Sybrandy, K. References Alborzi, Z.,
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. 2022 Jul;27(4):e12939.
It's a very "fun" ECG, with initial ectopic atrialtachycardia (negative P waves in inferior leads conducting 1:1 with the QRSs), followed by spontaneous resolution to sinus rhythm. Unfortunately the patient was erroneously diagnosed with "SVT / atrialfibrillation" and put on apixaban!!! What About the Tachycardia?
Abstract Introduction The use of flecainide and propafenone for medical cardioversion of atrialfibrillation (AF) and atrial flutter/intra-atrial reentrant tachycardia (IART) is well-described in adults without congenital heart disease (CHD). The unit of analysis was each episode of AF/IART.
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Recently diagnosed with intermittent paroxysmal atrialfibrillation but no EKGs available to confirm. Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Sinus tachycardia does not go this fast.
Artifact can obscure the rhythm or cause misdiagnosis of rhythms such as atrialfibrillation, ventricular tachycardia, and ventricular fibrillation. Instead — lead III tells us that the underlying rhythm is sinus tachycardia at 100-105/minute.
ACUTE MI (I allowed Acute MI to be in the report because I knew there would be an elevated troponin from ischemia, which is the definition of acute MI -- but in this case it would most likely be a Type 2 MI from tachycardia) There is also LA-RA lead reversal. The April 17, 2022 post ( Leads V1,V2 misplacement ). She had some fractures.
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrial flutter with regular conduction. Now the patient is in sinus tachycardia. Her initial EKG is below. Adenosine worked.
The ECG there reportedly showed an irregular tachycardia, and the patient was immediately referred to the emergency room. Here is her ECG on arrival: There is a wide complex tachycardia that is irregularly irregular (this is difficult to determine at these very high rates). Lead aVR seems to show the atrial activity clearly.
Written by Bobby Nicholson MD, with edits by Meyers A woman in her 50s with past medical history of heart failure, prior stroke, atrialfibrillation on Eliquis, lung cancer in remission, and CKD, presented to the emergency department for evaluation of cough and shortness of breath. What do you think? References: 1. Khouzam RN.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrialfibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. A normal PR interval.
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
AF Often Asymptomatic: Even for atrialfibrillation (AF)the most commonly symptomatic arrhythmiaover half of all cases were asymptomatic. Its estimated that undiagnosed atrialfibrillation alone costs the U.S. $3 Published March 24, 2022. Accessed April 25, 2024. link] 5 Ataklte et al. 2013;112(8):1263-1270.
BACKGROUND:Patients undergoing first-time atrialfibrillation (AF) ablation can benefit from targeting non-pulmonary vein (PV) triggers. Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Preprocedural identification of high-risk individuals can guide planning of ablation strategy.
The team immediately paged cardiology, concerned for polymorphic ventricular tachycardia. Since sinus conducted QRS complexes cannot co-exist together with ventricular tachycardia, this must all be artifact. Such as atrialfibrillation or sinus rhythm with extrasystoles. The October 21, 2022 post — for " artifactual VT".
Still more are factors are age < 18 years, sudden cardiac death in first degree relative, SCN5A mutations, atrialfibrillation, PR interval > 200 ms, QRS duration > 120 ms, presence of late potentials and aVR sign, manifested as R wave ≥ 0.3 2022 Mar;8(3):386-405. Atrialfibrillation and Brugada syndrome.
The rhythm is atrialfibrillation. If you use quantitative end-tidal CO2 monitoring, there is never any need to waste time making sure that the endotracheal tube is correctly placed. == MY Comment, by K EN G RAUER, MD ( 10/10/2022 ): == Today’s case is a “Save”! The QRS complex is within normal limits.
BackgroundIn medical practice, atrialfibrillation (AF) is intricately associated with heart failure (HF). The primary composite endpoint was defined as recurrence of atrialtachycardia over 30 s. AF patients received 4-step ablation composed of EIVOM, pulmonary vein isolation (PVI) and linear ablation. vs. 93.9%).
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. However, there is also significant tachycardia , with heart rate of 116, and known hypoxia. increasing stenosis, ischemia, volume changes, increased blood pressure, atrialfibrillation, etc.)
The relationship between J wave and ventricular tachycardia during Takotsubo cardiomyopathy. Prominent J waves and ventricular fibrillation caused by myocarditis and pericarditis after BNT162b2 mRNA COVID-19 vaccination. Can J Cardiol 2022 Kukla P, Jastrezebski M, Praefort W.
2:34 PM, following right heart catheterization She then went into atrialfibrillation with complete heart block and junctional escape rhythm prompting placement of transvenous pacemaker. Defibrillation strategies for refractory ventricular fibrillation. Case discussion: This is a tragic case. link] Bai, J., Tang, Z., &
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content