This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
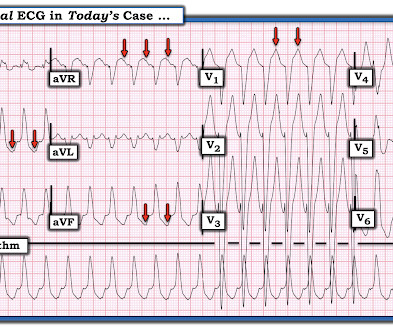
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation.
Introduction A high recurrence rate of atrial fibrillation was monitored after catheter ablation for persistent atrial fibrillation. Trial Registration Registered with Chinese Clinical Trials Registry on 27 August 2022, identifier: ChiCTR2200062995.
The standardized workflow included general anesthesia, a single transeptal puncture trough with a bidirectional, steerable visualizable sheath introduced into the left atrium accommodated a high density, penta-spline mapping catheter and a contact force sensor ablation catheter enabled to deliver vHPSD.
Abstract Introduction The utility of ablation index (AI) to guide ventricular tachycardia (VT) ablation in patients with structural heart disease is unknown. Methods Consecutive patients ( n = 103) undergoing initial VT ablation at a single center from 2017 to 2022 were evaluated.
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. The patient was started on amiodarone, anticoagulation, and metoprolol, and scheduled for atrial flutter ablation. He underwent ablation in the EP Lab.
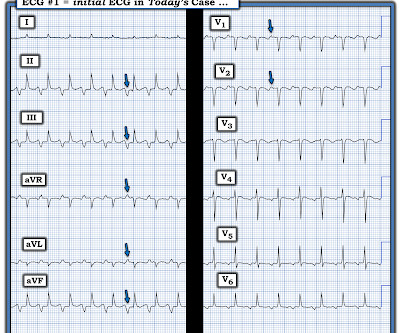
You are shown the ECG in Figure-1 — told only that the patient had a “continuous" tachycardia. PEARL # 4: This less common form of "fast-slow" AVNRT that is illustrated in Figure-3 — has also been known as an "incessant" tachycardia. QUESTIONS: How would YOU interpret the ECG in Figure-1 ? What is the differential diagnosis?
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrial flutter with regular conduction. Now the patient is in sinus tachycardia. Her initial EKG is below. Same as initial ECG.
Here is his ED ECG: Regular Wide Complex Tachycardia at a rate of 229 First : What do you want to do? Before getting into analysis, a regular wide complex tachycardia could be 1. ventricular tachycardia ( VT ) or 2. AV reciprocating tachycardia ( AVRT , antidromic WPW) or 3. Next : What do you think is the ECG diagnosis?
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). Meyers and Smith illustrate 20 example cases vs "look-alikes" of Swirl ( with my synthesis of "Swirl" ECG findings in My Comment on that post ) from October 15, 2022.
The ECG there reportedly showed an irregular tachycardia, and the patient was immediately referred to the emergency room. Here is her ECG on arrival: There is a wide complex tachycardia that is irregularly irregular (this is difficult to determine at these very high rates). Vitals were within normal limits other than heart rate.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chest pain and SOB. That said, against acute PE — is the inconstancy of this patient's symptoms — the lack of tachycardia — and the lack of any other ECG signs of acute RV strain. This was sent by a colleague.
BACKGROUND:Patients undergoing first-time atrial fibrillation (AF) ablation can benefit from targeting non-pulmonary vein (PV) triggers. Preprocedural identification of high-risk individuals can guide planning of ablation strategy. Among all first-time AF ablations, 68.1% were intermediate-risk (score 2, 10.5% risk), and 14.1%
Currently, ethanol infusion of vein of Marshall (EIVOM) for AF ablation in HF patients remains significantly limited.MethodThis was a non-randomized, single-center, retrospective observational study. AF patients received 4-step ablation composed of EIVOM, pulmonary vein isolation (PVI) and linear ablation. vs. 93.9%).
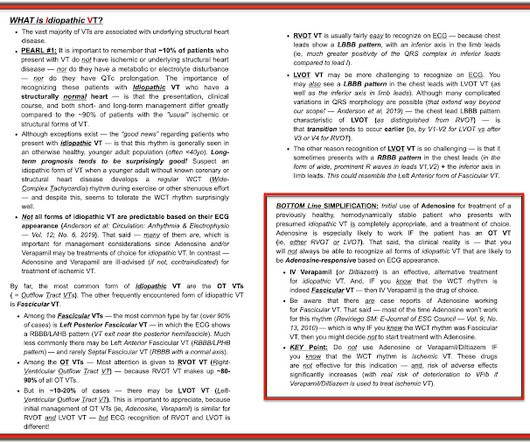
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). The patient has been scheduled for a PVC ablation procedure. This patient very likely has some form of idiopathic ventricular tachycardia. Potassium and magnesium serum levels were normal.
The CASE Continues: The patient had many episodes of NSVT ( Non-Sustained Ventricular Tachycardia ) — like th e one shown below in Figure-6. See "Lesson #3" in My Comment at the bottom of the page of the April 2, 2022 post for more on the diagnostic value of fusion beats ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content