This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. The rhythm is regular — at a rate just over 100/minute = sinus tachycardia ( ie, the R-R interval is just under 3 large boxes in duration ). Continuing with assessment of ECG #1 in Figure-2: The rhythm is sinus tachycardia at ~110/minute.
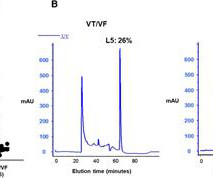
Background Early ventricular tachycardia/fibrillation (VT/VF) in patients with ST-elevation myocardial infarction (STEMI) has higher morbidity and mortality. This study examines gender-differentiated risk factors and underlying mechanisms for early onset VT/VF in STEMI. vs. 61.0 ± 13.0 vs. n = 46, L5: 4.3 ± 9.9%, P = 0.016).
This is ischemic ST depression, and could be due to increasing tachycardia, with a heart rate over 130, but that is unlikely given that the patient is now complaining of crushing chest pain and that there was tachycardia all along. There is widespread ST depression. Figure-1: Comparison of the first 2 ECGs in today's case.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). The below ECG was recorded. He required multiple defibrillations within a period of a few hours.
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 This is sinus tachycardia (rhythm) with complete heart block (AV node function) with ventricular escape rate just below 30. Never forget that sinus tachycardia is the scariest arrhythmia. What do you think?
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. 2] But there is also Sinus Tachycardia! Then, three minutes later… Crews activated STEMI as she deteriorated into PEA arrest. Closer inspection will show that it is Sinus, after all.
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". After initiating treatment for hyperkalemia, repeat ECG showed resolution of Brugada pattern: The ECG shows sinus tachycardia. A Very Wide Complex Tachycardia. The November 27, 2021 post ( LA-RA reversal ). What is the Rhythm?
pre-existing, stable atherosclerosis) amidst any state of global duress – to include hypertension, hypoxia, tachycardia, hypotension, sepsis, and GI bleed, for example. STEMI was activated and the patient went to Cath on arrival. There may even be significant overlap between these factors. Journal of Electrocardiology, 61 ; 41-46. [3]
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." As the troponin T was 1521 ng/L (peak troponin T over 1000 ng/L is typical of STEMI) and still rising, no further troponins were measured. Did YOU Notice that the underlying rhythm in Figure-1 appears to be atrial tachycardia?
A 12-lead was recorded, showing "STEMI," but is unavailable. There was never ventricular fibrillation (VF) or ventricular tachycardia (VT), no shockable rhythm. Here is a similar case: Collapse, Ventricular Tachycardia, Cardioverted, Comatose on Arrival. Agitation, Confusion, and Unusual Wide Complex Tachycardia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content