This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
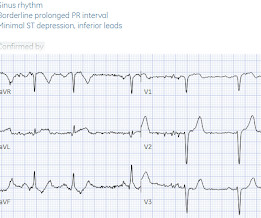
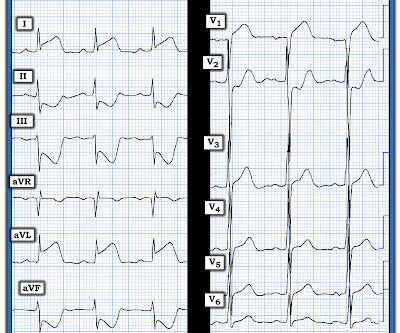
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion). The rhythm in ECG #1 is regular and supraventricular at a rate of ~75/minute.
Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. To Emphasize: The phenomenon of T-QRS-D is not needed in today's case to recognize the acute STEMI. The decision of whether to cath patients with a less definitive post-ROSC ECG is less clear.
This is a re-post of an excellent case from 2021. She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence. Here is the EM decision making: "The patient's EKG revealed some repolarization abnormalities but no clear signs of a STEMI. Chest x-ray was normal.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management. What is the gold standard for ECG interpretation: patient outcome!!!
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardial infarction (STEMI). There are conflicting sources regarding the relationship between hyperglycemia and outcomes in STEMI patients. 3.45) and 4.47 (95% CI: 2.54–7.87),
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al. Circulation. 2017;135(16):1490–3.
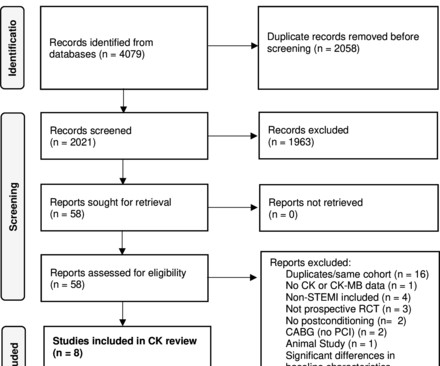
Objectives This study aimed to perform a meta-analysis of the short-term impact of ischaemic postconditioning (IPoC) on myocardial injury in ST elevation myocardial infarction (STEMI) using surrogate cardiac biomarkers. Conclusions IPoC does not seem to protect against myocardial injury in STEMI, except possibly in smokers.
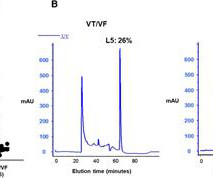
Background Early ventricular tachycardia/fibrillation (VT/VF) in patients with ST-elevation myocardial infarction (STEMI) has higher morbidity and mortality. This study examines gender-differentiated risk factors and underlying mechanisms for early onset VT/VF in STEMI. vs. 61.0 ± 13.0 years old, P = 0.008) with a male predominance.
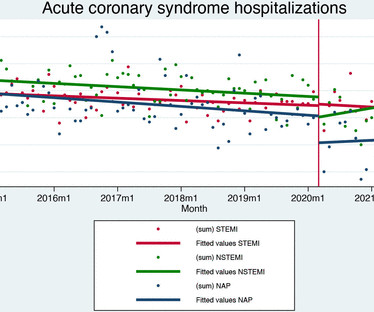
Methods and results Data for all patients admitted to hospital care for acute coronary syndromes in Slovenia (nationwide cohort) between 2014 and 2021 were obtained by merging the national hospital database, national medicines reimbursement database and population mortality registry using unique identifying numbers.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
Purpose Construction of a prediction model to predict the risk of major adverse cardiovascular events (MACE) in the long term after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardial infarction (STEMI).
P utting I t A ll T ogether : After correcting for LA-LL lead reversal — ECG # 1a shows sinus rhythm — LVH — and an acute infero-postero STEMI with acute RV involvement. PEARL # 3: In the absence of an anterior STEMI — acute inferior MI is the result of either acute RCA or LCx ( L eft C ircumfle x ) coronary occlusion.
Objectives To ascertain whether invasive assessment of coronary physiology soon after recanalisation of the culprit artery by primary percutaneous coronary intervention is associated with the development of microvascular obstruction by cardiac magnetic resonance in patients with ST-segment elevation myocardial infarction (STEMI).
So we activated the Cath Lab Angiogram: Impression and Recommendations: Culprit for the patient's anterior ST segment myocardial infarction and out of hospital V-fib cardiac arrest is a thrombotic occlusion of the mid LAD The first troponin returned barely elevated at 36 ng/L (URL = 35) In our study of initial troponin in STEMI, 26.8%
Another overlooked OMI ( Cardiologist limited by STEMI Definition — OMI evident by Mirror Test ) — See My Comment at the bottom of the page in the September 21, 2020 post on Dr. Smith’s ECG Blog. ECG Media Pearl # 8 ( 8:20 minutes Video ) — ECG Blog #191 — Distinguishing between A V D issociation vs Complete AV Block ( 2/6/2021 ).
There is an obvious inferior posterior STEMI(+) OMI. Methods Retrospective study of consecutive inferior STEMI , comparing ECGs of patients with, to those without, RVMI, as determined by angiographic coronary occlusion proximal to the RV marginal branch. The November 27, 2021 post ( LA-RA reversal ). What is the atrial activity?
Patients were selected from the HCA database (Jan 2021-Jul 2023). Patients with documented STEMI, left ventricular thrombus, mechanical mitral or aortic valve replacement were excluded. ICD 10 codes were used to identify patients with documented a fib. Procedure ICD codes were used to identify patients that underwent percutaneous LAAO.
That said, when you do see inverted U waves ( as we do in ECG #1 ) — this is a significant marker of severe ischemia ( Duque-Gonzálex et al — Cardiovascular Metal Sci 32(4), 2021 ). T oday's C ASE C ontinues: The worrisome findings in ECG #1 were recognized. The initial Troponin came back significantly elevated.
20% of cases that everyone would call a STEMI have a competely open artery by the time of angiogram 60-90 minutes later. PEARL #2: = Aslanger's Pattern: Examples of Aslanger's Pattern appear in a number of cases in Dr. Smith's ECG Blog ( This pattern is very nicely described by Dr. Smith in the January 4, 2021 post).
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Am J Med 2021 5. Moumneh T, Sun BC, Baecker A, et al. Lancet 2015 6.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al. Circulation. 2017;135(16):1490–3.
Epub 2021 Nov 17. These include about 60 occlusion MI (OMI) with clear ST segment elevation (none of which would be called “Normal” by the computer) and about 165 Non-STEMI. Of the Non-STEMI in our cohort, about 25% will actually have acute coronary occlusion. Am J Emerg Med. 2022 Jan;51:384-387. doi: 10.1016/j.ajem.2021.11.023.
Here is the repeat ECG at 52 minutes after arrival to triage: Obvious posterolateral STEMI Angiographic findings: 1. page 1932 • “The application of STEMI ECG criteria on a standard 12-lead ECG alone will miss a significant minority of patients who have acute coronary occlusion. (21) Left main: no significant stenosis.
From My Comment in the November 15, 2023 post in Dr. Smith's ECG Blog: Clinical Points about MINOCA: Given the literature citing a 5-15% estimated incidence of MINOCA in patients initially diagosed as having a STEMI or "NSTEMI" — it is important to be aware of the more common entities associated with this entity ( See Figure-2 ).
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 The November 27, 2021 post ( LA-RA reversal ). What do you think? Although not necessarily intentional, the first processing that I do when I see an ECG is to categorize as OMI or not. mm STE in V2).
Smith and Meyers to diagnose both obvious (STEMI) and subtle OMI. NOTE: For detailed review regarding use of Cardiac MRI in acute chest pain evaluation — See the extensive article by Broncano et al ( RadioGraphics 41:8-31, 2021 ). It was trained by Drs. The young age always makes one suspicious of myocarditis.
2021 Dec 7;10(23):e022866. Epub 2021 Nov 15. Recall that air is a poor conductor of electricity and will, therefore, generate smaller amplitudes on posterior leads (hence why STEMI criteria requires only >0.5 J Am Heart Assoc. doi: 10.1161/JAHA.121.022866. 121.022866. mm in any posterior lead to be considered positive).
2021 Sep;49(6):488-500. Aslanger EK, Meyers HP, Smith SW. Recognizing electrocardiographically subtle occlusion myocardial infarction and differentiating it from mimics: Ten steps to or away from cath lab. Turk Kardiyol Dern Ars. doi: 10.5543/tkda.2021.21026. 2021.21026. Among the important points brought out by Dr.
2021 Dec 7;10(23):e022866. Epub 2021 Nov 15. Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia). J Am Heart Assoc. doi: 10.1161/JAHA.121.022866. 121.022866. PMID: 34775811; PMCID: PMC9075358. Aslanger EK. J Electrocardiol.
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. If this patient was managed according to the STEMI/NSTEMI paradigm (although he would be a candidate for early invasive treatment), he would probably be taken to the cath lab hours later. 2021 Sep;49(6):488-500. Turk Kardiyol Dern Ars. doi: 10.5543/tkda.2021.21026.
Background:The computational pressure-fluid dynamics applied to index of microcirculatory resistance, derived from coronary angiography (CPFD-caIMR) is a promising alternative method of IMR to evaluate the prognosis of STEMI patients. All patients with STEMI underwent CPFD-caIMR and MVO assessment.
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." As the troponin T was 1521 ng/L (peak troponin T over 1000 ng/L is typical of STEMI) and still rising, no further troponins were measured. How does the Queen of Hearts do? Ann Emerg Med [Internet].
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). Annals of Emergency Medicine 2021. Triage ECG: What do you think?
The primary safety end point was Bleeding Academic Research Consortium 3 to 5 bleeding at 30 days.RESULTS:Between January 10, 2019, and September 18, 2021, a total of 2989 patients were randomized. The primary efficacy end point occurred in 37 patients (2.5%) in both the PPA and placebo groups (hazard ratio, 1.00 [95% CI, 0.63 to 1.57]).
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chest pain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. The below ECG was recorded.
BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI. The EMS crews were correct moving forward with STEMI activation. 1] Driver, B.
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. Then, three minutes later… Crews activated STEMI as she deteriorated into PEA arrest. A finger-stick glucose resulted 551 mg/dL, and the following ECG was recorded. & Schocken, D.
STEMI was activated and the patient went to Cath on arrival. The distribution of findings is consistent with the LAD, of which is now open with improved TIMI flow. The ECG’s were sent to the PCI center, and the providers in the respective ED identified the T wave characteristics mentioned above. Journal of Electrocardiology, 61 ; 41-46. [3]
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content