This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardialinfarction (STEMI). There are conflicting sources regarding the relationship between hyperglycemia and outcomes in STEMI patients.
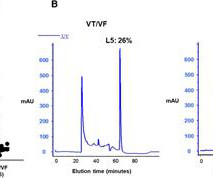
Background Early ventricular tachycardia/fibrillation (VT/VF) in patients with ST-elevation myocardialinfarction (STEMI) has higher morbidity and mortality. This study examines gender-differentiated risk factors and underlying mechanisms for early onset VT/VF in STEMI. vs. 61.0 ± 13.0 vs. 1.70 ± 0.28, P = 0.02
Objectives This study aimed to perform a meta-analysis of the short-term impact of ischaemic postconditioning (IPoC) on myocardial injury in ST elevation myocardialinfarction (STEMI) using surrogate cardiac biomarkers. These results resonate with some studies using imaging techniques to ascertain myocardial damage.
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Objectives To ascertain whether invasive assessment of coronary physiology soon after recanalisation of the culprit artery by primary percutaneous coronary intervention is associated with the development of microvascular obstruction by cardiac magnetic resonance in patients with ST-segment elevation myocardialinfarction (STEMI).
Purpose Construction of a prediction model to predict the risk of major adverse cardiovascular events (MACE) in the long term after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardialinfarction (STEMI).
associated typical MyocardialInfarction therapies such as statins and ACE inhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. MINOCA I do not have the bandwidth here to write a review of MINOCA.
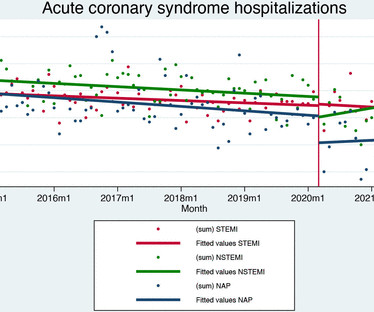
Methods and results Data for all patients admitted to hospital care for acute coronary syndromes in Slovenia (nationwide cohort) between 2014 and 2021 were obtained by merging the national hospital database, national medicines reimbursement database and population mortality registry using unique identifying numbers.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
There is an obvious inferior posterior STEMI(+) OMI. Literature cited In inferior myocardialinfarction, neither ST elevation in lead V1 nor ST depression in lead I are reliable findings for the diagnosis of right ventricular infarction Johanna E. What is the atrial activity? Is it sinus arrest with junctional escape?
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Aslanger's pattern (Smith was co-author on this): A new electrocardiographic pattern indicating inferior myocardialinfarction The next troponin returned at 8822 ng/L. 20% of cases that everyone would call a STEMI have a competely open artery by the time of angiogram 60-90 minutes later.
So we activated the Cath Lab Angiogram: Impression and Recommendations: Culprit for the patient's anterior ST segment myocardialinfarction and out of hospital V-fib cardiac arrest is a thrombotic occlusion of the mid LAD The first troponin returned barely elevated at 36 ng/L (URL = 35) In our study of initial troponin in STEMI, 26.8%
Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. It can only be seen by IVUS.
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Am J Med 2021 5. Shah ASV, Anand A, Sandoval Y, et al. Lancet 2015 6.
The ECG in ER is shown below: ECG is still diagnostic but we are watching the natural course of myocardialinfarction here. Considerations on the naming of myocardialinfarctions. 2021 Sep;49(6):488-500. He arrived to our hospital one hour later. J Electrocardiol. 2022 Mar-Apr;71:44-46. doi: 10.1016/j.jelectrocard.2022.01.006.
Although not striking, this is clearly a diagnostic ECG for infero"posterior" myocardialinfarction due to coronary occlusion (OMI), most likely due to left circumflex (LCx) artery occlusion. mm STE even in the fourth universal definition of myocardialinfarction. 2021 Dec 7;10(23):e022866. Epub 2021 Nov 15.
Epub 2021 Nov 17. Available from: [link] Excerpt: "To illustrate the limitations imposed by sample size, recent data from our institution reveal that we identify approximately 225 type I myocardialinfarctions (MI) in a typical year. Of the Non-STEMI in our cohort, about 25% will actually have acute coronary occlusion.
Here is the repeat ECG at 52 minutes after arrival to triage: Obvious posterolateral STEMI Angiographic findings: 1. page 1932 • “The application of STEMI ECG criteria on a standard 12-lead ECG alone will miss a significant minority of patients who have acute coronary occlusion. (21) Left main: no significant stenosis.
See our publication: ST depression in lead aVL differentiates inferior ST-elevation myocardialinfarction from pericarditis There is STE in inferior leads, high lateral leads, and V4-V6. Smith and Meyers to diagnose both obvious (STEMI) and subtle OMI. And there is ST depression in V2 and V3, all but diagnostic of posterior OMI.
Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion MyocardialInfarction (Versus Nonocclusive Ischemia). 2021 Dec 7;10(23):e022866. Epub 2021 Nov 15. J Am Heart Assoc. doi: 10.1161/JAHA.121.022866. 121.022866. mm in any posterior lead to be considered positive).
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
Smith , d and Muzaffer Değertekin a DIFOCCULT: DIagnostic accuracy oF electrocardiogram for acute coronary OCClUsion resuLTing in myocardialinfarction. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. 2021 Sep;49(6):488-500. Here is the post-intervention angiogram and post-PCI ECG. 2021.21026.
Patients with ST-segment–elevation myocardialinfarction undergoing primary percutaneous coronary intervention were randomly assigned by center to receive low-dose PPA or matching placebo for at least 48 hours. mg·kg·h of bivalirudin intravenously). mg·kg·h of bivalirudin intravenously). to 1.57]).
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." Immediate and early percutaneous coronary intervention in very high risk and high risk non-ST segment elevation myocardialinfarction patients. How does the Queen of Hearts do? Ann Emerg Med [Internet]. 2012;60:766–776. 2023;131569.
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). Annals of Emergency Medicine 2021. Triage ECG: What do you think?
BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI. The EMS crews were correct moving forward with STEMI activation. 1] Driver, B.
His father and brother both died of myocardialinfarction at ages 61 and 45, respectively. STEMI was activated and the patient went to Cath on arrival. New insights into the use of the 12 Lead Electrocardiogram for diagnosing Acute MyocardialInfarction in the emergency department. 2] Aslanger, E., 3] deWinter, R.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). The below ECG was recorded. Inotropic medication was continued.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content