This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
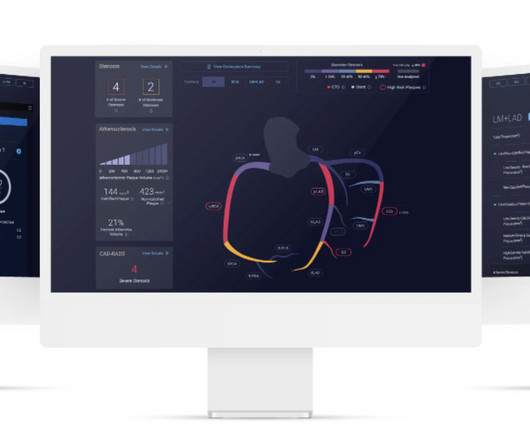
The study describes the validation of Cleerly's artificial intelligence-guided quantitative coronary CT angiography (AI-QCT) ISCHEMIA technology for diagnostic accuracy and prognostic risk stratification. High Diagnostic Accuracy of AI-ISCHEMIA in Comparison to PET, FFR-CT, SPECT, and Invasive FFR: A Pacific Substudy. 2024.01.007.
6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. Diagnosis and treatment of ischemia-producing coronary stenoses improves 5-year survival of patients undergoing major vascular surgery.” 2021, [link].
TIB in the intervention group was significantly reduced at the 1,2, and 4-week marks post-intervention and exhibited a higher effective rate of total myocardial ischemia load reduction. The control group underwent a standard rehabilitation program, while the intervention group participated in an individualized exercise rehabilitation program.
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. Hence the first ECG was labeled 'anterior ischemia' based on ST depression, rather than identifying this as reciprocal from posterior OMI. Curr Cardiol Red 2021 3. J Am Heart Assoc 2021 6.
Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. That this is all demand ischemia is unlikely. Lung exam showed diffuse B lines bilaterally. Aslanger's pattern.
If left untreated, PAD may progress to severe forms known as chronic limb-threatening ischemia (CLTI) and acute limb ischemia (ALI). It has been estimated that less than 5% of patients with PAD in the U.S. are prescribed to participate in a supervised exercise program.”
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiac arrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). To EMPHASIZE: This pattern of diffuse Subendocardial Ischemia does not suggest acute coronary occlusion ( ie, it is not the pattern of an acute MI ).
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] There is evolution from Wellens Pattern A to Pattern B, now inclusive of V6.
There is no definite evidence of acute ischemia. (ie, Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. ( Some residual ischemia in the infarct border might still be present. Both episodes are initiated by an "R-on-T" phenomenon.
This observational cohort study investigates clinical approaches and long-term outcomes of iatrogenic CeAD after endovascular interventions.Methods:We conducted a retrospective chart review to analyze patients who underwent endovascular treatments at the Mayo Clinic from 1998 to 2021. Pertinent patient factors were extracted.
Introduction:Tenecteplase (TNK) is becoming the preferred thrombolytic for acute brain ischemia. A six-month lead-in, six-month introductory, and one-year transition period began in April 2021 using an intentional change method. We subsequently educated constituents including nursing, pharmacy, technical and clinical staff.
As a result — IF no "fixable" cause is found ( ie, ischemia/infarction — electrolyte disturbance — rate-slowing medication ) — then because of the AV block and very slow heart rate, this patient will probably need a pacemaker. There are also twice as many P waves as QRS complexes — so at the least, there is 2nd-degree AV block.
2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. The absence of STE in V7-V9 is often due to resolution of ischemia, as seen by resolution of ST depression in V7-V9. non-occlusive ischemia) JAHA 2021 3. -- Meyers HP, Bracey A, Lee D, et al.
My interpretation was: RBBB with hyperacute T-waves in V4-V6 that are all but diagnostic of LAD occlusion vs. post ROSC ischemia. The patient had ROSC and maintained it. A 12-lead ECG was obtained: What do you think? Smith's ECG Blog — Interpretation of a post-resuscitation ECG can be extremely challenging.
ACUTE MI (I allowed Acute MI to be in the report because I knew there would be an elevated troponin from ischemia, which is the definition of acute MI -- but in this case it would most likely be a Type 2 MI from tachycardia) There is also LA-RA lead reversal. The November 27, 2021 post ( LA-RA reversal ).
We performed this analysis to identify the prevalence of atrial fibrillation and associated outcomes in symptomatic internal carotid artery stenosis patients undergoing CAS or CEA.Methods:We analyzed the data from the National inpatient sample (NIS) between January 2016 to December 2021. versus 18.8% for CAS or CEA, respectively, p=0.50].
This suggests further severe ischemia. There is 1 mm of ST segment elevation in lead aVR — which in the context of ST segment flattening in most other leads, suggests that there may be a component of subendocardial ischemia from underlying coronary disease. Detailed coronary artery evaluation not performed. Downstream vasospasm?
Objective:To assess whether diffusion restriction (DR) of the retina and optic nerve (ON) can be accurately and reliably identified on standard stroke protocol brain magnetic resonance diffusion-weighted imaging (DWI-MRI) in patients presenting with acute non-arteritic central retinal artery occlusion (CRAO).Background:Retinal
Am J Med 2021 5. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines JACC 2021 8. Was this objective evidence of inducible ischemia accompanied by chest pain?
Background:COVID-19, primarily a respiratory illness caused by SARS-CoV-2, is associated with vascular complications like ischemia due to endothelial injury, hypercoagulability, and inflammation. A subgroup analysis was conducted for patients during the vaccination period (April 14, 2021, to March 1, 2022).
The outcome measure was peri-procedural complications defined as a composite of perioperative death, major bleeding, contrast nephropathy, myocardial infarction, ischemic stroke, and major amputation. Notable comorbidities included diabetes mellitus at 60.6% and dialysis at 29.9%, respectively. of the participants.
A majority (62.5%) of those presenting with ‘normal’ ECGs had the cath lab activated without any ECG being labeled ‘STEMI’ by automated interpretation – based on signs of Occlusion MI including ECG changes, regional wall motion abnormality on bedside ultrasound, or refractory ischemia. 2021 ; 46 : 23 - 26 4. Acad Emerg Med.
In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) I interpret tracings systematically in "real time" ( including my assessment for acute ischemia ). The November 27, 2021 post ( LA-RA reversal ). The rate is near 80, normal.
The right TRA was performed as a first-line approach from 2019 to 2021, with the left TRA being used thereafter. Patients who underwent proximal balloon-protected CAS were excluded. We analyzed patient characteristics, clinical outcomes, and the presence of lesions on postprocedural diffusion-weighted imaging (DWI lesions).Results:A
Remote ischemic conditioning (RIC) with transient ischemia and reperfusion applied to the arm has been shown to accelerate hematoma resolution in both animal and clinical studies. Results:Between Apr 22, 2021, and Oct 30, 2023, 458 patients were randomly assigned, with 229 in each group. 13.0), and the median hematoma volume was 12.6
Stroke, Volume 55, Issue Suppl_1 , Page A48-A48, February 1, 2024. Objective:To compare the 1-month stroke, myocardial infarction (MI), and/or death rates among symptomatic patients undergoing either CAS or CEA according to the timing of the procedure in Carotid Revascularization Endarterectomy versus Stenting Trial (CREST).Methods:We
Traditional methods of non-invasive ischemia testing (stress EKG , stress echo, SPECT , PET , direct-to-cath) can result in false negatives 20-30 percent of the time, which can lead to undetected disease, and false positives over 50 percent of the time, which can lead to unnecessary invasive procedures. 2021 ACC/AHA Chest Pain Guidelines.
This is critical for the EMS provider, or ED clinician, as identification of Grade I ischemia (aka, HATW’s) addresses the culprit lesion at the earliest opportunity with excellent downstream prognosis for the patient. [2] Chapter 6: Introduction to Myocardial Ischemia and Infarction. 2] But there is also Sinus Tachycardia!
And superimposed subendocardial ischemia pattern, of course. A number of potentially severe pulmonary complications t hat convey higher morbidity and mortality are commonly seen in patients with CTD ( Taha and Feteih — NIH, Skills in Rheumatology, 2021 ). She was otherwise very stable during this rhythm.
There is no ischemia, certainly no concern at all for OMI. These ER patients did not have ischemia — and the variation in ST elevation was not related to either heart rate or QRS amplitudes ( Variation in ST-Segment Elevation in Early Repolarization: Electrocardiography 40:10,2007 ).
Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). Figure-3: Diagnostic considerations for a patient who presents in AV block ( adapted from Mangi et al — StatPearls, 2021 ). Usually the medical history will provide clues to the cause.
See Costagliola et al — Ann Clin Transl Neurol 8(7): 1557-1568, 2021 — for more on the complex "Brain-Heart Interaction" in Epilepsy ). mEq/L for K+ and 1.76 Over the years, I have found recall of a short LIST of Causes of QT Prolongation to be of invaluable assistance.
When “spot diagnosing” precordial ST-depression I instinctively evaluate aVR for any corresponding ST-elevation to see if an emerging pattern of broad subendocardial ischemia can be appreciated, in which the ST-depression should be otherwise global and demonstrably maximal in Leads II and V5. ST-elevation, etc.) is present. 5] Meyers, H.
Common explanations for unusual rhythms such as this one include: i ) Hyperkalemia ( or other severe electrolyte disorder ); ii ) Recent infarction/ischemia; iii ) Sleep apnea; iv ) Severe hypothyroidism; v ) Acute neurologic catastrophe (ie, stroke, bleed, trauma, tumor ); vi ) Some other toxicity. Narcan was not given at the scene.
In most cases, rather, the culprit is gross ischemia due to myocardial infarction, cardiomyopathy, or advanced coronary artery disease. Unfortunately, today’s case is lacking any such diagnostics, thus I cannot say with certainty that the QT interval is, or is not, culpable in arrhythmogenesis. [1] Wolters-Kluwer: Philadelphia, PA. [2]
Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia). 2021 Dec 7;10(23):e022866. Epub 2021 Nov 15. J Am Heart Assoc. doi: 10.1161/JAHA.121.022866. 121.022866.
This suggests ischemia of uncertain duration. The October 25, 2021 post in Dr. Smith's ECG Blog — My Comment ( at the bottom of the page ) reviews my approach to another case of a Dual-Level Wenckebach block. There is deep, symmetric T wave inversion with a prolonged QTc interval in anterior leads V1,V2,V3.
If you still have not read it, I strongly recommend that you read the following article on the diagnosis of "posterior" MI: Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia), by Meyers HP et al. 2021 Dec 7;10(23):e022866.
mg reduced the risk of cardiovascular death, MI or heart attack, ischemic stroke, or ischemia-driven coronary revascularization by 31% compared with placebo.34 2021 Apr 20;77(15):1958-1959]. This in turn leads to an overall reduction in IL-6 production and CRP concentration.12 12 Colchicine, 0.5 34 Colchicine, 0.5 J Am Coll Cardiol.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Lead V2 shows RR’ QRS configuration, and although ST depression is otherwise expected here, the discordance is a bit excessive. 6] Tabrizi, F.,
Annals of Emergency Medicine 2021. EKG shown here: LAFB with no clear signs of OMI or ischemia. Electrocardiographic Diagnosis of Acute Coronary Occlusion Myocardial Infarction in Ventricular Paced Rhythm Using the Modified Sgarbossa Criteria. In which we compared ventricular paced OMIs with Non-OMIs and MI-ruled out patients.
These include ( among others ) — acute febrile illness — variations in autonomic tone — hypothermia — ischemia/infarction/cardiac arrest — and Hyperkalemia. The November 27, 2021 post ( LA-RA reversal ). PEARL # 5: A number of conditions other than Brugada Syndrome may temporarily produce a Brugada-1 ECG pattern.
Figure-2: Classification of Underlying Diagnoses in Patients with MINOCA ( Adapted from Table-1 in Sykes et al: Interventional Cardiology Review: 16:e10, 2021 ).
The outcome was arterial thromboembolism (ischemic stroke, embolism of extremity, or transient cerebral ischemia). Female sex was not considered a risk factor in any risk group.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content