This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
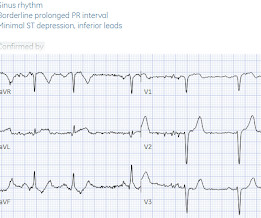
Written by Jesse McLaren, with a very few edits by Smith A 60-year-old presented with chestpain. The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. But STEMI criteria is only 43% sensitive for OMI.[1]
Written by Jesse McLaren A 50 year old presented to triage with one hour of chestpain, and the following ECG labeled normal by the computer (GE Marquette SL) algorithm. Smith comment: we showed that the first troponin, even in full-blown STEMI, is negative 25% of the time. What do you think?
Written by Jesse McLaren A previously healthy 60 year old developed exertional chestpain with diaphoresis, and called EMS. So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. What do you think?
Written by Jesse McLaren Four patients presented with chestpain. 4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6]
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset. Epub 2021 Nov 17. 2021.11.023.
Written by Jesse McLaren Two 70 year olds had acute chestpain with nausea and shortness of breath, and called paramedics. There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD.
A 50-something man presented in shock with severe chestpain. There is an obvious inferior posterior STEMI(+) OMI. Methods Retrospective study of consecutive inferior STEMI , comparing ECGs of patients with, to those without, RVMI, as determined by angiographic coronary occlusion proximal to the RV marginal branch.
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. Smith and Meyers to diagnose both obvious (STEMI) and subtle OMI. But the stuttering pain and sudden onset suggest acute coronary occlusion (Occlusion MI, or OMI). No pericardial effusion on ultrasound."
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. 2021 Dec 7;10(23):e022866. Epub 2021 Nov 15. Triage EKG: What do you think? J Am Heart Assoc. 121.022866.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Am J Med 2021 5. Int J Cardiol 2013 2.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. Limkakeng AT.
Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion). The rhythm in ECG #1 is regular and supraventricular at a rate of ~75/minute.
Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. To Emphasize: The phenomenon of T-QRS-D is not needed in today's case to recognize the acute STEMI. Once the J-point is recognized in the chest leads ( RED arrows in leads V2,V3,V4 of Figure-2 ) — the marked ST elevation becomes obvious.
The pain was completely resolved after coronary intervention. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. If this patient was managed according to the STEMI/NSTEMI paradigm (although he would be a candidate for early invasive treatment), he would probably be taken to the cath lab hours later.
This is a re-post of an excellent case from 2021. A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. He had active chestpain at the time of triage at 0137 at night, with this triage ECG: What do you think?
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest. He was treated for infection and DKA and admission to hospital was planned.
So we activated the Cath Lab Angiogram: Impression and Recommendations: Culprit for the patient's anterior ST segment myocardial infarction and out of hospital V-fib cardiac arrest is a thrombotic occlusion of the mid LAD The first troponin returned barely elevated at 36 ng/L (URL = 35) In our study of initial troponin in STEMI, 26.8%
Having looked for negative U waves in patients with chestpain over a period of decades — I'll emphasize that this is not a common finding. That said, when you do see inverted U waves ( as we do in ECG #1 ) — this is a significant marker of severe ischemia ( Duque-Gonzálex et al — Cardiovascular Metal Sci 32(4), 2021 ).
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. Step 1 to missing posterior MI is relying on the STEMI criteria. But it is still STEMI negative. What do you think? A 15 lead ECG was done (below).
If you saw this ECG only knowing that it is an acute chestpain patient, what would be your interpretation? However, in the context of the first ECG and the waning chestpain, this is diagnostic of reperfusion. Due to the severity of the pain and the high BP, they obtained an aortic dissection CT.
Figure-1: The initial ECG in today's case — obtained from a 50-year old man with new chestpain. ( The deep anterior S waves and tall lateral chest lead R waves suggest significant LVH. The November 27, 2021 post ( LA-RA reversal ). How many of these findings can YOU identify? HINT: Is the rhythm sinus ?
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. 2021 Sep;49(6):488-500. STE in lead I and II are more subtle. A second ECG was taken at 15:16. Wait for the angiogram.
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. What is it?
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
A 40 something otherwise healthy man presented with substernal chestpain. Epub 2021 Nov 17. These include about 60 occlusion MI (OMI) with clear ST segment elevation (none of which would be called “Normal” by the computer) and about 165 Non-STEMI. It had occurred once 3 days prior and resolved without any medical visit.
Case A 39-year-old male without prior medical history presents with chestpain that started 2 hours prior to presentation. He says that the pain intensity was 10/10 at home but now about 4/10. Despite the clinical stability and decreasing pain, this patient needs an immediate angiogram. 2021 Dec 7;10(23):e022866.
Written by Jesse McLaren Two patients presented with acute chestpain, and below are the precordial leads V1-6 for each. Patient 1 Patient 2 STEMI criteria is based only ST elevation millimeter criteria measured in isolation from the QRS and stratified by age/sex, so this is the only information provided above.
Written by Pendell Meyers, with edits by Smith A man in his 80s presented with acute chestpain and normal vital signs. It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." 2021;Available from: [link] Other references: Lindow T, Mokhtari A, Nyström A, Koul S, Smith SW, Ekelund U.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content