This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest. See this post: What do you think the echocardiogram shows in this case?
Formal Echocardiogram: Normal left ventricular size and wall thickness. For example — Baldi et al note a more than doubling in the number of false-positive ECGs for STEMI i f judgments were based on post-resuscitation 12-lead tracings obtained less than 7 minutes after ROSC ( Resuscitation 162:445-446, 2021 ).
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. His echocardiogram showed normal wall motion.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
Case A 39-year-old male without prior medical history presents with chestpain that started 2 hours prior to presentation. He says that the pain intensity was 10/10 at home but now about 4/10. Despite the clinical stability and decreasing pain, this patient needs an immediate angiogram. 2021 Dec 7;10(23):e022866.
A 40 something otherwise healthy man presented with substernal chestpain. Formal Echocardiogram: The estimated left ventricular ejection fraction is 58 %. Epub 2021 Nov 17. It had occurred once 3 days prior and resolved without any medical visit. What do you think? This ECG is DIAGNOSTIC of acute LAD Occlusion.
His medical history is unremarkable except a similar pain occurred 4-5 times in the previous 3 months with less intensity, short duration, unrelated to exertion. He visited an outpatient clinic for it and an echocardiogram and exercise stress test was normal. 2021 Sep;49(6):488-500. He has 40 packs-year of smoking history.
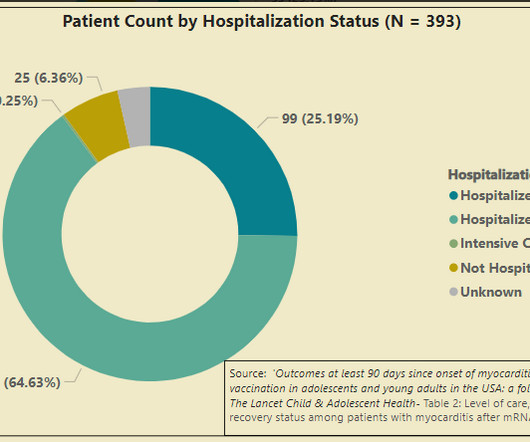
In August 2021, the CDC began a study to follow-up cases of myocarditis in the age group at highest risk for myocarditis after mRNA COVID-19 vaccination. I have to make the obligatory post-script here that I oversaw the administration of hundreds of mrna vaccines starting in March of 2021 in my cardiology clinic.
He was concerned because he had chestpain after his first mRNA vaccine and was uncomfortable with the risks of a second mRNA dose. He received his first dose of a Pfizer mRNA COVID19 vaccine in June 2021. He subsequently describes having sharp chestpain over the next few weeks. As I discussed with Mr.
He played a round of golf a week prior and felt an episode of chestpain during the round, which spontaneously resolved. On presentation, he reported no chestpain or shortness of breath. Five days later, the patient was exercising when he developed chestpain at 19:30 which lasted for an hour.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content