This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Jesse McLaren, with a very few edits by Smith A 60-year-old presented with chestpain. Inferior hyperacute T waves, which have been added to the 2022 ACC consensus on chestpain as a “STEMI equivalent”[3] 3. Curr Cardiol Red 2021 3. J Am Heart Assoc 2021 6. IJC Heart and Vasc 2021 8.
Written by Jesse McLaren Four patients presented with chestpain. 2021 ; 46 : 23 - 26 4. All initial ECGs were labeled ‘normal’ or ‘otherwise normal’ by the computer interpretation, and below are the ECGs with the final cardiology interpretation. Villarroel NA , Houghton CJ , Mader SC , Poronsky KE , Deutsch AL , Mader TJ.
Whenever a patient does not have chestpain, the pre-test probability of OMI is diminished. Of course SOB, jaw pain, shoulder pain, etc can be a result of OMI, but the pretest probability is less and so you must scrutinize further. Here is the first ED ECG: COMPUTER INTERPRETATION: Electronic Atrial Pacemaker.
Written by Jesse McLaren A 50 year old presented to triage with one hour of chestpain, and the following ECG labeled normal by the computer (GE Marquette SL) algorithm. 2021 ; 46 : 23 - 26. What do you think? Theres normal sinus rhythm, first degree AV block, early R wave, normal voltages. Here is her ECG: What do you think?
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset. Epub 2021 Nov 17. 2021.11.023.
A 50-something man presented in shock with severe chestpain. The November 27, 2021 post ( LA-RA reversal ). His prehospital ECG was diagnostic of inferior posterior OMI. The patient was in clinical shock with a lactate of 8. He appeared gray in color, with cool skin. The February 11, 2020 post ( LA-RA reversal ).
Written by Jesse McLaren A previously healthy 60 year old developed exertional chestpain with diaphoresis, and called EMS. Here’s the EMS ECG, digitized with PM cardio. What do you think? There’s sinus arrhythmia with normal conduction, normal axis and normal voltages. There’s loss of R waves in V2-3 with hyperacute waves V1-5.
This interest may be attributed in part to a 2021 decision by the American College of Cardiology (ACC) and the American Heart Association (AHA) to give cardiac CT angiography (CCTA) its highest recommendation as a frontline test to evaluate patients with stable and acute chestpain who have no history of coronary artery disease.¹
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. PEARL: Most patients who present with new chestpain + ECG changes + positive troponin — will not need Cardiac MRI. This was sent to me by a partner: "Curious what you think of this one we had overnight.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. 2021 Dec 7;10(23):e022866. Epub 2021 Nov 15. Triage EKG: What do you think? J Am Heart Assoc. 121.022866.
5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 2021, [link]. JAMA Internal Medicine, vol. 1071, [link]. 22, 30 Nov.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Am J Med 2021 5. Int J Cardiol 2013 2.
Written by Jesse McLaren Two 70 year olds had acute chestpain with nausea and shortness of breath, and called paramedics. Int J Cardiol Heart Vasc 2021 2. Today's patient is a 70-year old adult who called EMS because of new-onset chestpain , associated with nausea and shortness of breath. Who needs the cath lab?
BACKGROUND:The PRECISE (Prospective Randomized Trial of the Optimal Evaluation of Cardiac Symptoms and Revascularization) demonstrated that a precision diagnostic strategy reduced the primary composite of death, nonfatal myocardial infarction, or catheterization without obstructive coronary artery disease by 65% in patients with nonacute chestpain (..)
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Annals of Emergency Medicine 2021. Triage ECG: What do you think? This is diagnostic of proximal LAD occlusion.
2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of ChestPain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. 2021 Nov 30;144(22):e368-e454. Epub ahead of print. PMID: 38483420. Circulation.
Methods We prospectively included 1384 patients with LRHSs between March 2019 and March 2021. Therefore, this study aims to investigate the value of NISI in risk stratification and predicting cardiac events in patients with low-risk HEART scores (LRHSs).
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest. He was treated for infection and DKA and admission to hospital was planned.
TheNational Institute for Health and Care Excellence(NICE) recommends CCTA as the first-line investigation for patients with chestpain due to suspected CAD, highlighting its importance in improving diagnostic certainty. June 11, 2021. link] iv IMV.2023 2023 CTMarket Outlook Report (p. v Walter, M. 2024,November 8).
As discussed in detail in ECG Blog #228 — this seemingly qualifies as a “ Silent ” MI ( Approximately half of those MIs not accompanied by CP — have some other associated symptom such as syncope, which substitutes as a “chestpain equivalent” ).
For example — Baldi et al note a more than doubling in the number of false-positive ECGs for STEMI i f judgments were based on post-resuscitation 12-lead tracings obtained less than 7 minutes after ROSC ( Resuscitation 162:445-446, 2021 ).
Today's case is also noteworthy in that T-QRS-D is seen in association with RBBB — which has only been described on rare occasions ( See the March 28, 2021 post i n Dr. Smith's ECG Blog ). Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. He became unconscious on arrival.
Having looked for negative U waves in patients with chestpain over a period of decades — I'll emphasize that this is not a common finding. That said, when you do see inverted U waves ( as we do in ECG #1 ) — this is a significant marker of severe ischemia ( Duque-Gonzálex et al — Cardiovascular Metal Sci 32(4), 2021 ).
Impression: In this middle-aged man with palpitations and dyspnea, but no chestpain — I suspect that the T wave peaking and slight, upward-sloping chest lead ST elevation represent a repolarization variant. The November 27, 2021 post ( LA-RA reversal ). The March 18, 2020 post ( LA-RA reversal ).
This is a re-post of an excellent case from 2021. A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. He had active chestpain at the time of triage at 0137 at night, with this triage ECG: What do you think?
Ella Dunmore, who is a mother and former soldier, made the decision to seek medical attention, she had been experiencing headaches, chestpain, and shortness of breath for several weeks. Dr. Kaki implanted Impella CP® on March 18, 2021, while he cleared blockages and inserted stents. Thought to share about it.
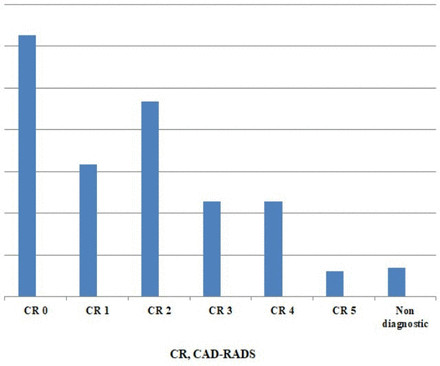
Methods RLCCTS started October 2021 using a wide detector array CT system, with 20 min slots. Six months of data were collected; stable chestpain (SCP) patients, who have national CTCA QC comparators, were analysed using descriptive statistics. Uncertain CAD-RADS meant a non-diagnostic scan (NDS).
years]) admitted to the China ChestPain Center Database between 2016 and 2021. Hierarchical clustering of 15 medical conditions was performed to derive multimorbidity patterns. The primary outcome was a composite of inhospital adverse events.
a med tech company dedicated to helping patients with persistent ischemic heart disease, has announced the treatment of the first patient with the A-FLUX Reducer System, a treatment for patients with angina or chestpain. 27 May 2021. VahatiCor, Inc., Angina is often caused by reduced blood flow to the heart. Circulation.
If you saw this ECG only knowing that it is an acute chestpain patient, what would be your interpretation? However, in the context of the first ECG and the waning chestpain, this is diagnostic of reperfusion. Due to the severity of the pain and the high BP, they obtained an aortic dissection CT.
With more than 500 peer-reviewed publications, the HeartFlow FFR CT Analysis remains unparalleled in precision coronary care, as supported by the ACC/AHA ChestPain Guidelines, to improve treatment plans and outcomes. 2021 ACC/AHA ChestPain Guidelines. For more information: www.heartflow.com References 1.
Sometimes arrhythmogenic cardiomyopathy patients can present with acute chestpain and elevation of myocardial enzymes and has been called as ‘hot phase’ These require differentiation from acute myocardial infarction and have normal coronary arteries [3]. 2021 Jun 7;23(6):907-917. doi: 10.1093/europace/euaa343.
Cardiac Cath labs waiting for some major influx of COVID heart damage not only didn’t see patients presenting with COVID heart attacks, but they idled as patients terrified of coming to the hospital stayed home rather than come to the hospital with chestpain. But the politics was all pervasive. Anish Koka is a Cardiologist.
we analyzed patients presenting from 2016 to 2021 with an initial diagnosis of stroke, defined by ICD-10 codes in any diagnostic position as abstracted from free text responses by ED staff. We therefore used population-level data to report the frequency of cardiac troponin assessments among U.S. 32.2%) had troponin tested in the ED.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
A 2021 study published in Radiology: Cardiothoracic Imaging focused on cardiac imaging trends over a decade. Standardized terminology allows for consistency in communication across all members of the imaging community and will assist with clinical care and multicenter trials.”
We can argue endlessly about what exactly the risk of COVID19 was in the Spring of 2020, or 2021, but there should be little argument in 2023 that the risks of COVID pneumonia striking down a young healthy individual is now extremely low. Notice that there is no spike in myocarditis diagnoses until the second half of 2021.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
She was hemodynamically stable — and did not have chestpain, lightheadedness or syncope. The October 25, 2021 post in Dr. Smith's ECG Blog — My Comment ( at the bottom of the page ) reviews my approach to another case of a Dual-Level Wenckebach block. QUESTIONS: HOW would you interpret the rhythm in Figure-1 ?
2021 Sep 15;339:219-224. “ If there ain’t no plaque, there ain’t no heart attack ” When used to assess those presenting with chestpain, the use of CTCA led to a 41% reduction in the risk of future major heart events, including heart attacks and death from coronary artery disease 2. Int J Cardiol.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. 2021 Sep;49(6):488-500. STE in lead I and II are more subtle. A second ECG was taken at 15:16. Wait for the angiogram.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content