This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
My thoughts were the following: ECGs #1 and #2 showed a completely unreliable sinus pacemaker, with presumed high-grade 2nd-degree AV block — and frequent resultant pauses of over 2 seconds ( that would have been even longer had it not been for intermittent relief from the atrial escape focus ). What Does this All Mean?
Is a pacemaker needed? Even if we stopped here — We could conclude the following: There is marked bradycardia in today's rhythm ( ie, Heart rate in the low 30s ). Finally — If today's patient does not have significant underlying coronary disease — then her bradycardia with AV block may be the result of SSS ( S ick S inus S yndrome ).
Looking first at the long-lead II rhythm strip — there is significant bradycardia , with a heart R ate just under 40/minute. The patient may need a pacemaker. But the point to emphasize — is that it should only take seconds to recognize that there is bradycardia from significant AV block. =
There was no evidence bradycardia leading up to the runs of PMVT ( as tends to occur with Torsades ). If there had been — a temporary atrial pacemaker could have been considered as a way of increasing the heart rate to suppress a bradycardia-dependent arrhythmia ("overdrive pacing").
That said — obvious findings include: i ) Marked bradycardia! — My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. The rhythm in Figure-1 is complex — and defies precise interpretation without careful study. be regular! —
Abstract Introduction Severe transitory episodes of bradycardia with subsequent syncope in children are common, and generally portend a benign prognosis. Patients with SP or AVB, 21 years of age or younger, who underwent CNA between 2015 and 2021 were included. Methods This is a single-center, case series study. The median age was 18.9
Isoprenalin was discontinued, and a temporary transveous pacemaker was implanted. The patient stabilized following pacemaker placement. For example — bradycardia and AV conduction disturbances are not uncommon with Hyperkalemia , with these conduction disturbances most often resolving once serum K+ is corrected.
He received a permanent pacemaker during the subsequent inpatient stay. plaque disruption), the T waves still manifest markings of a previous state of suboptimal coronary flow that resolved: Type II supply-demand mismatch in the setting of extreme bradycardia. Hospital transport was unremarkable. 6] Tabrizi, F., 7] Callans, D.
To improve visualization — I've digitized the original ECG using PMcardio ) MY Thoughts on the ECG in Figure-1: This is a challenging tracing to interpret — because there is marked bradycardia with an irregular rhythm and a change in QRS morphology. Figure-1: The initial ECG in today's case. ( The QRS complex is wide ( ie, >0.10
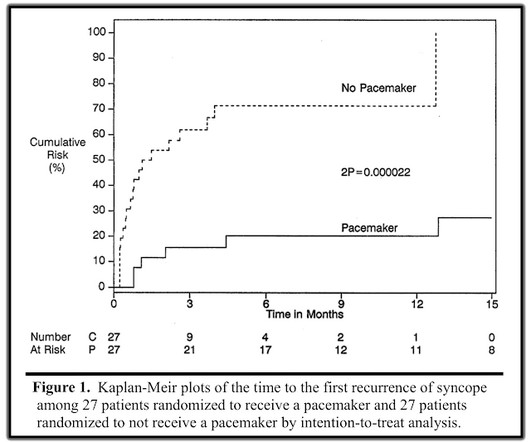
If the block is not vagal in nature, the patient should receive a pacemaker. There was a randomized trial to determine whether pacemakers could benefit patients with vasovagal syncope, aptly named The North American Vasovagal Pacemaker Study (VPS). In the repeat study (VPS II), EVERY patient had an implanted pacemaker.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content