This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
With P waves labeled — Isn't it now much easier to appreciate that the atrial rhythm is quite regular ( with no more than a slight sinus arrhythmia )? P utting I t A ll T ogether : The precise mechanism of today's arrhythmia is complex and difficult to determine. For those with a special interest in cardiac arrhythmias — READ ON! —
Krantz et al authored a State-of-the-Art Review on Cardiovascular Complications of Opioid Use ( JACC 77(2):205-223, 2021 ) — in which mechanisms from Opioid Overdose that detail arrhythmia production ( up to cardiac arrest ) are elucidated — thereby providing an explanation for the unusual arrhythmias in today's case.
However, he suddenly developed a series of malignant ventricular arrhythmias. Below are printouts of some of the arrhythmias recorded. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. The arrhythmia starts with a PVC having a short coupling interval.
Looking first at the long-lead II rhythm strip — there is significant bradycardia , with a heart R ate just under 40/minute. But the point to emphasize — is that it should only take seconds to recognize that there is bradycardia from significant AV block. = Would you approve her for a nonemergent surgical procedure?
VT is the second most common presenting arrhythmia. Vaso or inotropic medications are not harmless, and can precipitate life threatening arrhythmias. It is common with 2nd- and 3rd-degree AV block to see a " ventriculophasic " sinus arrhythmia. AV block is the first manifestation of CS in more than 30% of patients.
KEY Point: Knowing that the most commonly overlooked arrhythmia is AFlutter — suggests that the BEST way to avoid missing the diagnosis of AFlutter is simply to THINK of AFlutter whenever you have a regular SVT at a rate close to 150/minute ( in which you do not clearly see upright sinus P waves in lead II ).
That said — obvious findings include: i ) Marked bradycardia! — L addergram I llustration : At this point — I needed to work out, and then draw a laddergram that I could then verify to ensure a plausible mechanism for today's arrhythmia. The rhythm in Figure-1 is complex — and defies precise interpretation without careful study.
Details of management extend beyond the scope of this ECG Blog — with reviews by Atemnkeng at al ( J Med Cases 12[9]:373-376, 2021 ) and Chakraborty & Hamilton ( StatPearls, 2023 ) available for interested readers. It's always rewarding and mutually educational to discuss interesting aspects of arrhythmia interpretation.
plaque disruption), the T waves still manifest markings of a previous state of suboptimal coronary flow that resolved: Type II supply-demand mismatch in the setting of extreme bradycardia. Chapter 17: Ventricular Arrhythmias. 2] Although the clinical context in today’s case does not fit these descriptors for Type I OMI (e.g.
To improve visualization — I've digitized the original ECG using PMcardio ) MY Thoughts on the ECG in Figure-1: This is a challenging tracing to interpret — because there is marked bradycardia with an irregular rhythm and a change in QRS morphology. Was there a family history of sudden death or significant arrhythmia?
A repeat ECG was performed as adult cardiology was asked to evaluate the patient for emerget PCI: Sinus bradycardia with persistent elevation in the inferior leads with reciprocal depression in aVL Patient was taken to cath lab with adult cardiology which revealed normal coronary arteries without evidence of occlusion MI. Epub 2021 Jul 7.
The possibility of an ischemic cause of the ventricular arrhythmia has to be considered! Below in Figure-5 is a 10-minute continuous lead II recording on oral Flecainide, now showing sinus bradycardia without a single PVC! A workup was undertaken in search of a cause of the patient's ventricular arrhythmia. No PVCs are seen.
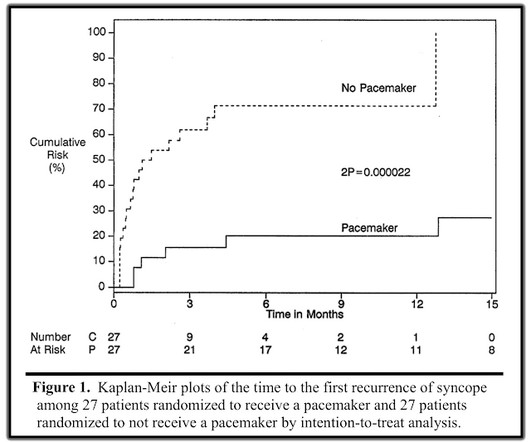
Perhaps because the bradycardia in vasovagal syncope is only one part of the autonomic response. Phase 4 block is also referred to as "bradycardia dependent block." A stunning result. One of many examples in medical history that remind us of the importance of blinding in clinical trials. Why was there no benefit? link] Lee, S.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content