This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
There is a regular narrow complex tachycardia. Thus, it is supraventricular tachycardia. It is important to remember that SVT includes Sinus Tachycardia! Sometimes even Wide Complex Tachycardia is Sinus. See this case in which Lewis leads were necessary to figure this out: Wide Complex Tachycardia.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation. What to do?
QUESTIONS: Is this rhythm too fast to be sinus tachycardia? However, until such time that we know for certain — I think it best to simply describe what we see: PEARL # 1: Realize that for any tachycardia — there are 6 Parameters that need to be assessed. Are flutter waves hidden within the QRS and T waves? s in Figure-2 ).
Working through a case of a regular WCT Rhythm in this 80-something woman See My Comment in the May 5, 2020 post on Dr. Smiths ECG Blog. Another case of a regular WCT Rhythm in a 60-something woman See My Comment at the bottom of the page in the April 15, 2020 post on Dr. Smiths ECG Blog. Smiths ECG Blog.
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. While today's case is the first we have published on cardiac sarcoidosis — we have featured infiltrative cardiomyopathy ( ie, with amyloidosis — in the November 15, 2020 post in Dr. Smith's ECG Blog ).
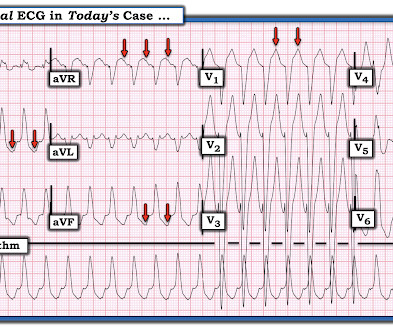
IMPRESSION: Given the presence of a wide tachycardia — with 2 distinct QRS morphologies, and no sign of P waves — a presumed diagnosis of B i D irectional Ventricular Tachycardia has to be made. See My Comment in the June 1, 2020 post in Dr. Smith's ECG Blog — for review of Pleomorphic VT.
On the monitor patient had wide-complex tachycardia. Differential is ventricular tachycardia versus supraventricular tachycardia with aberrancy versus sinus tachycardia with a aberrancy. After the patient was stabilized with supportive care, the heart rate gradually slowed, confirming sinus tachycardia.
Introduction:Supraventricular tachycardia (SVT) is known to affect children and teenagers predominantly but can also occur in adults. in adults (above 25 years) from 1999 to 2020. in adults (above 25 years) from 1999 to 2020. Results:From1999 to 2020, 31,036 (AAMR=0.6) in 2020 (APC 13.66). in 2020 (APC 13.66).
His previous echo one month prior shows the same thing: “consistent with old infarct in LAD vascular territory, with EF 45%” "I think there is something else causing his tachycardia which is exaggerating his EKG findings and mimicking an acute myocardial infarction." The patient spontaneously converted back to sinus tachycardia.
Abstract Introduction Supraventricular tachycardia (SVT) is a common pediatric arrhythmia. Individuals aged 1–21 years at time of SVT diagnosis initiated on a BB or a CCB between 01/01/2010 and 12/31/2020 were included. Exclusion criteria were pre-excitation, ectopic atrial tachycardia, and hemodynamically significant heart disease.
It's a very "fun" ECG, with initial ectopic atrial tachycardia (negative P waves in inferior leads conducting 1:1 with the QRSs), followed by spontaneous resolution to sinus rhythm. What About the Tachycardia? Today's regular SVT rhythm could be an ectopic atrial tachycardia ( ATach ) — or an automatic junctional tachycardia.
Here is her ED ECG: Here is the ED physician's interpretation: IMPRESSION UNCERTAIN REGULAR RHYTHM, wide complex tachycardia, likely p-waves. LEFT BUNDLE BRANCH BLOCK [120+ ms QRS DURATION, 80+ ms Q/S IN V1/V2, 85+ ms R IN I/aVL/V5/V6] Comparison Summary: LBBB and tachycardia are new. This is clearly ventricular tachycardia.
Short-long-short (S-L-S) electrocardiographic cycle length patterns are associated with incidence of ventricular tachycardia (VT) and ventricular fibrillation (VF). It is also recognised that pacemakers can facilitate these cycle length sequences, and that the observation of these sequences can predict future VT/VF events.
There is a regular wide complex tachycardia. Remember : Adenosine is safe in Regular Wide Complex Tachycardia. Rather, from this one: Very Fast Very Wide Complex Tachycardia Ideally, one would cardiovert. An older patient with no previous medical history arrived at triage complaining of SOB. If it is VT, there will be no effect.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. Analysis: there is a wide complex tachycardia. This was the interpretation I put into the system: WIDE COMPLEX TACHYCARDIA. It is regular.
RBBB is no longer seen after conversion to sinus rhythm — which supports our suspicion that the intermittent RBBB conduction seen every-other-beat during the tachycardia ( in Figure-1 ) was rate-related. Note that QRS morphology after conversion to sinus rhythm is very similar to QRS morphology of odd-numbered beats during the tachycardia.
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
Multifocal Atrial Tachycardia 2. of all cases, and 62% of Veritas® misdiagnoses). == MY Comment , by K EN G RAUER, MD ( 1/5/2020 ): == This case illustrates a number of important teaching points. The rhythm is indeed irregularly irregular, so atrial fibrillation must be considered. Sinus with multifocal PACs 3.
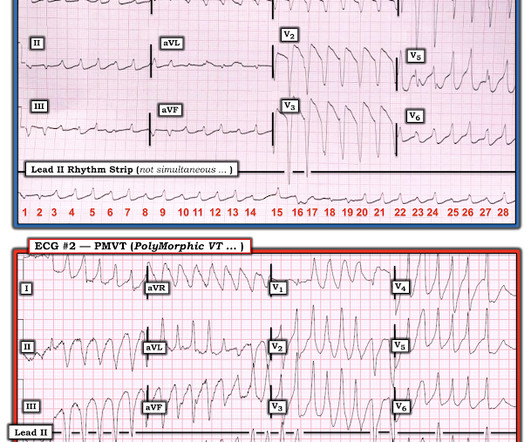
== MY Comment by K EN G RAUER, MD ( 6/1 /2020 ): == YOU are asked to interpret the ECG shown in Figure-1. When PMVT is associated with a long QT interval — the rhythm is then defined as Torsades de Pointes ( Please SEE My Comment at the bottom of the April 29, 2020 post in Dr. Smith’s ECG Blog ). Figure-1: The initial ECG in the ED.
QUESTIONS: Is the wide tachycardia that is seen best in the chest leads, too irregular to be VT ( V entricular T achycardia )? — For more on the diagnostic significance of identifying AV dissociation in wide tachycardia — See ECG Blog #133 and ECG Blog #151. How certain are YOU of your answer?
NOTE: The ECGs in today's case are recorded in the Cabrera Format ( See Dr. Grauer Comment in the October 26, 2020 post of Dr. Smith's ECG Blog for review on the Cabrera Format ). The 2019 ESC Guidelines for the management of patients with supraventricular tachycardia indicated that IV Amiodarone should not be considered in these populations.
The team immediately paged cardiology, concerned for polymorphic ventricular tachycardia. Since sinus conducted QRS complexes cannot co-exist together with ventricular tachycardia, this must all be artifact. The November 10, 2020 post — for PTA. The October 17, 2020 post — for a 70-year old woman with " Artifactual VT ".
Retrospectively — I interpret this 1:1 retrograde conduction as diagnostic of a reentry SVT rhythm as the etiology of the initial tachycardia. Working through a case of a regular WCT Rhythm in this 80-something woman — See My Comment in the May 5, 2020 post on Dr. Smith’s ECG Blog.
Figure-1: Reasons for the varied ECG presentation of acute LMain occlusion — excerpted from Dr. Smith’s 8/9/2019 post ( This Table from My Comment in the January 16, 2020 post ). The ST-T wave appearance in lead aVR can be anything when there is acute LMain occlusion.
While the initial impression might not immediately suggest ventricular tachycardia (VT), a closer examination raises suspicion. Additionally, the qR morphology, particularly in a patient with right bundle branch block (RBBB) type wide QRS complex tachycardia (WQCT), lends further support for VT. What is the rhythm?
PEARL # 2: The way in which I look for flutter waves is to carefully set my calipers at precisely HALF the R-R interval o f the tachycardia ( since IF the rhythm is AFlutter — then the atrial rate should be twice the ventricular rate if there is 2:1 AV conduction ). See text ).
With normal EF the tachycardia is not compensatory. And the patient has sinus tachycardia. ( On arrival patient was slightly tachycardic. HR about 90-100/min. Other vital signs normal. Hand held echo showed overall ejection fraction being normal. ACS then becomes less likely. Final diagnosis was myocarditis. at ~100/minute ).
The rhythm is regular — at a rate just over 100/minute = sinus tachycardia ( ie, the R-R interval is just under 3 large boxes in duration ). Continuing with assessment of ECG #1 in Figure-2: The rhythm is sinus tachycardia at ~110/minute. Figure-2: I've labeled the initial ECG. The QRS complex is obviously wide.
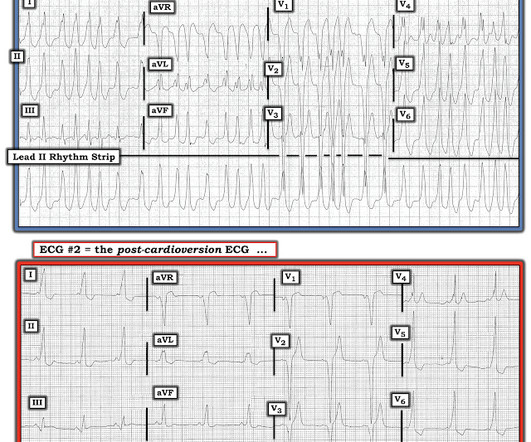
There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). This patient was having recurrent episodes of polymorphic ventricular tachycardia with an underlying long QT interval ( = Torsades des Pointes ). ECG #2 Interpretation of ECG #2: Underlying sinus rhythm.
All pediatrics presenting to AUBMC between 2000 and 2020 who underwent cardiac ablation were included. The remaining 15% of patients presented with less common types of arrhythmias, including other supraventricular tachycardias (SVTs), retrograde dual atrioventricular nodal reentry, and premature ventricular contractions (PVC).
MY Interpretation of Today's Initial ECG: I've labeled key findings in Figure-2 for today's initial ECG: The rhythm is sinus tachycardia at ~105/minute. The sinus tachycardia is a definite concern that something acute may be ongoing. Figure-2: I've labeled t he initial ECG. All intervals ( PR, QRS, QTc ) are normal.
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Sinus tachycardia does not go this fast. A 60-something ow healthy male had syncope while on treadmill. What do you want to do?
I focus my thoughts on a qualitative approach to these 3 pre-hospital ECGs — all obtained from patients presenting with acute CP ( C hest P ain ). == ECG #1 — from a 70-ish year old Woman with acute CP and Dyspnea The rhythm is sinus tachycardia at a surprisingly rapid rate of ~115/minute. Sometimes — You have to be there.
You are shown the ECG in Figure-1 — told only that the patient had a “continuous" tachycardia. PEARL # 4: This less common form of "fast-slow" AVNRT that is illustrated in Figure-3 — has also been known as an "incessant" tachycardia. ECG Blog #138 — AFlutter vs Atrial Tachycardia. What is the differential diagnosis?
This is sinus tachycardia (rhythm) with complete heart block (AV node function) with ventricular escape rate just below 30. Never forget that sinus tachycardia is the scariest arrhythmia. The February 11, 2020 post ( LA-RA reversal ). The March 18, 2020 post ( LA-RA reversal ). The August 28, 2020 post ( LA-LL reversal ).
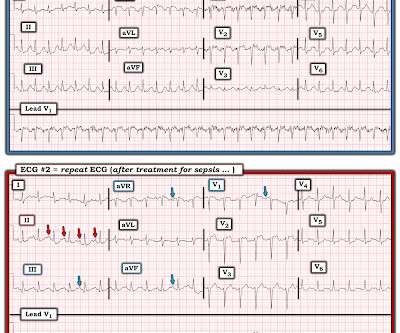
As I discuss in detail in My Comment at the bottom of the page in the May 24, 2020 post in Dr. Smith's ECG Blog — AV dissociation is not the same as AV block. ANSWER to the Challenge Question: Note that the rhythm in ECG #2 is sinus tachycardia at ~100-105/minute. PEARL # 5: Accelerated junctional rhythms are not common in adults.
But for those wanting a "simpler" approach" — Consider the following ( which I review below in my ADDENDUM ): This patient is in a wide, "ugly-looking" and seemingly regular tachycardia without P waves. Working through a case of a regular WCT Rhythm in this 80-something woman — See My Comment in the May 5, 2020 post on Dr. Smith’s ECG Blog.
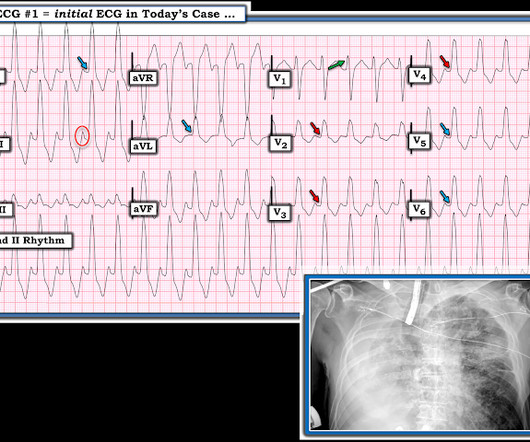
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). As I review in My Comment in the January 16, 2020 post of Dr. Smith's ECG Blog ( and have reproduced in Figure-2 below ) — the ECG of patients with acute LMCA occlusion may be varied.
Methods Patients were retrospectively evaluated between January 2012 and June 2020. Objectives To describe a cohort of patients with arrhythmogenic left ventricular cardiomyopathy (ALVC), focusing on the spectrum of the clinical presentations. Significant right ventricular involvement was an exclusion criterion.
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrial flutter with regular conduction. Now the patient is in sinus tachycardia. Her initial EKG is below. Same as initial ECG.
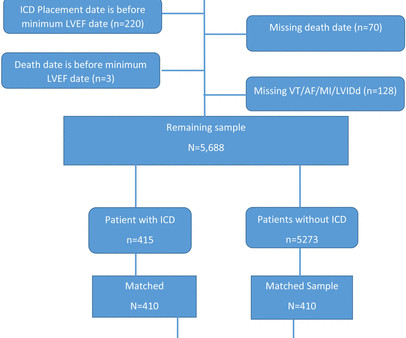
Methods Patients with lowest LVEF between 30% and 35% without an ICD prior to the lowest-LVEF echo (defined as ‘time zero’) were identified by querying echocardiography data from 28 November 2001 to 9 July 2020 at the Massachusetts General Hospital linked to ICD treatment status. vs 65.4%, p<0.0001), more often white (87.5%
This point is particularly relevant regarding ECG #2 — because sinus tachycardia is seen on this earlier ECG. In Figure-4 — I've reproduced from the above cited June 20, 2020 post my schematic illustration of the ST-T wave appearance that may be seen in one or more lateral leads for demonstrating LV "strain".
== MY Comment by K EN G RAUER, MD ( 3/12/2020 ): == A young adult presented to the ED with the “heart awareness” and the ECG shown in Figure-1 — but with no more than slight shortness of breath. DDx of Polymorphic wide tachycardia: 1. DDx of irregularly irregular wide complex tachycardia : 1. Wide complex tachycardia 2.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content