This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Introduction:For a subset of patients with acute ischemic stroke (AIS) with large vessel occlusion (LVO) mechanical thrombectomy with a stent retriever and/or aspiration is insufficient to revascularize the target artery. Rescue therapy with angioplasty alone or with stenting has been utilized.
Introduction:Medical therapy and endovascular therapy for intracranial atherosclerotic disease (ICAD) have evolved over the past two decades with improved medical therapy benchmarks, and improved techniques and patient selection for stenting. vs 10.2%) in the 2020 patient group compared to the 2009 patients. vs 7.9%), diabetes (33.6%
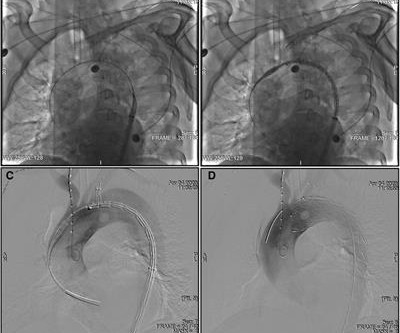
BackgroundThe left subclavian artery (LSA) can be intentionally covered by a stent graft to acquire adequate landing zones for a proximal entry tear near the LSA during thoracic endovascular aortic repair (TEVAR). The Castor single-branched stent graft is designed to treat type B aortic dissection (TBAD) to retain the LSA during TEVAR.
1 To date, interventional treatment of coronary artery disease with drug-eluting stents has been able to establish flow angiographically. 2 “For many years, it was thought that caging of the vessel with stents was the main driver for annual increasing non-plateauing event rates. JACC 2020. of the U.S. population.
BACKGROUNDRescue intracranial stenting (RICS) is increasingly recognized as a potentially effective rescue strategy following failed mechanical thrombectomy (MT) for large vessel occlusion due to intracranial atherosclerosis, but populationlevel data on contemporary patterns of RICS utilization in MT are lacking. had codes for MT.
BACKGROUND:In patients with post-thrombotic syndrome, stent recanalization of iliofemoral veins or the inferior vena cava can restore venous patency and improve functional outcomes. The risk of stent thrombosis is particularly increased during the first 6 months after intervention.
Herein, we describe a single‐step approach to deploy Neuroform Atlas stent (Stryker Neurovascular, Fremont, CA) which is a hybrid laser‐cut, nitinol self‐expanding stent without the need for ELW or lesion re‐access using MINI TREK RX (Abbott Vascular, Inc., There was no restriction on time from last known well (TLKW) to MT.
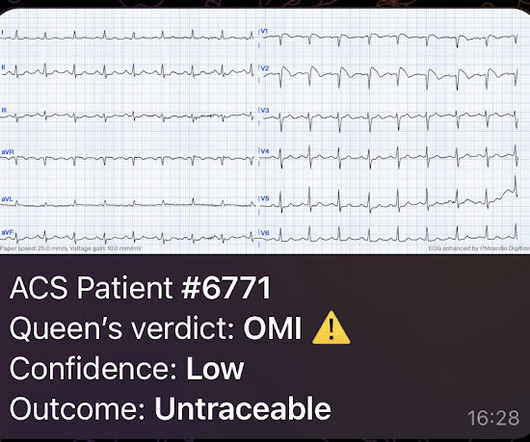
Angiogram: Widely patent RCA and LAD stents. Therefore, no stent was placed. (No It is proven better than angiography alone in stable angina , and also has been shown to improve decisions on stenting non-culprit lesions in ACS. We are told that this middle-aged male patient has a history of prior MI with stents.
Background:Persistent hypotension after carotid artery stenting (CAS) can lead to adverse outcomes, prolong length of stay (LOS), and increase hospital costs. A relation between decline of norepinephrine after stenting and persistent hypotension supports the role of catecholamine in BP control.
Purpose:Since the balloon protection device became unavailable in Japan three years ago, the DWI-positive rate after carotid artery stenting (CAS) has increased. Stroke, Volume 55, Issue Suppl_1 , Page ATMP68-ATMP68, February 1, 2024. Symptomatic stenosis (63.9% vs. 94.7%, p<0.05) was more common in the with-POWER group.
Introduction:Current evidence suggests that acute carotid artery stenting (CAS) for cervical lesions is associated with better functional outcomes in patients with acute stroke with tandem lesions (TLs) treated with endovascular treatment (EVT). Stroke, Volume 55, Issue Suppl_1 , Page ATMP94-ATMP94, February 1, 2024.
Recently, the ductus arteriosus stent (DAS) has become a viable alternative.Methods and ResultsThis was a retrospective multicenter study of neonates ≤30 days undergoing DAS or Blalock‐Taussig‐Thomas shunt placement between January 1, 2017 and December 31, 2020 at hospitals reporting to the Pediatric Health Information Systems database.
He next underwent stenting in his coronary arteries in 2000, 2010 and 2012 at Pune. A total of 6 stents were placed. Coronary angiography showed multiple blocks in the stents, needing an urgent bypass surgery. He himself developed heart disease a couple of years later. He recently developed unstable angina.
We also compared the safety of acute carotid stenting (CAS) in TLs with low ASPECTS.Methods:This prospective multicenter study from 16 centers included patients with anterior circulation TL from 2015-2020. in patients with stenting (18/44) versus no-stenting (25/44).Conclusion:This 3.05; p=0.32), PH2 (OR: 1.14, CI: 0.26-5.02;
We present the cumulative percutaneous coronary intervention (PCI) data of all comers (stable angina and acute coronary syndromes [ACS]) who presented to Hadi Clinic between January 2018 and December 2020. A total of 567 patients underwent coronary catheterisation for the three-year period between January 2018 and December 2020.
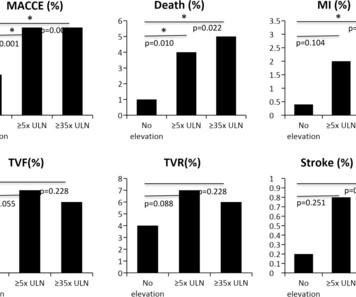
Methods Between September 2011 and April 2020, 726 patients undergoing CTO PCI at 2 Belgian referral centres were prospectively included and divided into 4 groups based on postprocedural hs-TnT levels (unelevated; ≥5 times the upper limit of normal (ULN); ≥35 times the ULN; ≥70 times the ULN).
Methods This retrospective study was conducted at a single center and involved 481 patients who received frozen elephant trunk stent implantation for TA-AAD. This study was performed at Fuwai Hospital between September 2016 and April 2020.
EKG from triage: Here is his previous ECG: Normal ST Elevation Resident's interpretation: Reperfusion pattern/Wellens' with biphasic T waves in V2 and V3, and in comparison to an EKG in 2020 this is new. Here are other very interesting posts: Wellens' syndrome: to stent or not?
One would not expect wall motion to recover so quickly after stenting, so this is good evidence that the POCUS echo was indeed accurate. The case I presented in My Comment to that March 9, 2020 post showed a patient with this pattern — who on cath had no more than minimal coronary disease.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. The patient was transferred to CCU to consider surgical options.
ml/h, P = 0.04), a higher likelihood of parent artery stenosis (65% vs. 20.8%, P < 0.001), and increased need for angioplasty or stenting (50% vs. 17%, P < 0.001). Follow-up lesion volumes and functional outcomes were similar; however, the mismatch group showed a slower infarct growth rate (3.8 ml/h vs. 7.5 vs. 21.2%, P = 0.02).Conclusions:DWI-ADC
The patient was found to have total "mid" LAD occlusion which was stented: Pre-PCI. Patient 2 Clinical Course and Outcome: This patients first ECG was sent to the EM physician who said it did not meet STEMI criteria, but wisely agreed with EMS to get serial ECGs during transport. The cath lab was now activated.
This led to immediate cath lab activation — which revealed total occlusion of a large 1st diagonal branch that was stented. == Below is the ECG of Patient #3 — recorded from a 35-year old man with sudden, new-onset CP. In a word — Patient #2 was lucky to have his ECG interpreted by the Queen Of Hearts. Sometimes — You have to be there.
The studies were classified in 3 periods by publication date: Period 1: before 2015, pre-stent retriever; Period 2: 2015-2019, early thrombectomy era; and Period 3: 2020-2024, recent period.Results:Of 2693 references, 21 trials met inclusion criteria, 3 in Period 1, 10 in Period 2, 8 in Period 3.
LAD and D1 were stented, but flow unfortunately could not be well restored despite efforts (they list the post intervention TIMI flow still as 0). Serial tracings following stent placement confirmed the large extent of myocardial injury. LCX and RCA were described as "normal" in the cath report. There is ST elevation in lead aVL.
IntroductionFlow diverters (FD) are stent‐type devices that enable the exclusion of intracranial aneurysms in clinical scenarios where coil‐type devices exhibit high failure rates. Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. Adults older than 18 with non‐ruptured intracranial aneurysms were included.
MT cases for strokes between 2020 and 2022 were reviewed. To be included, two or more passes of MT using stent retrievers in combination with aspiration must have occurred. Favorable functional outcomes were identified as mRS of 0 to 2 and NIHSS of 0 to 4 at discharge.
Just before 10 AM, the patient received a stent to the culprit OM. We know that today's patient has had prior inferior OMI with stenting of his proximal RCA ~3 years earlier. In this view, the culprit lesion is not particularly obvious which is an important principle in angiography, and the reason why we obtain multiple views.
Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. The February 11, 2020 post ( LA-RA reversal ). The March 18, 2020 post ( LA-RA reversal ). The August 28, 2020 post ( LA-LL reversal ). The November 19, 2020 post ( LA-LL reversal ). The July 29, 2018 post ( LA-RA reversal ).
Decision was made to stent the lesion. We review ECG findings in Takotsubo Cardiomyopathy in the March 25, 2020 post of Dr. Smith's ECG Blog. An echo was done and decision was made to pursue cath lab the following day as the echocardiography was interpreted as consistent with Takotsubo Cardiomyopathy.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The reappearance of de Winter's pattern caused by acute stent thrombosis: A case report. Am J Emerg Med. 2014;32:e5–e8. As per Drs.
Between 2020 and 2023, thirty cerebral aneurysms were treated with at least 80% utilization of the Balt Optima™ Coil System. Serious adverse events including, but not limited to, groin hematoma, periprocedural stroke, intraoperative aneurysm rupture, coil herniation requiring stent placement, and mortality were recorded.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. It was stented. He wrote most of it and I (Smith) edited. He had multiple episodes of bradycardia and nonsustained ventricular tachycardia. This was a large OMI.
Unfortunately, we do not have those images for review, but the operators described a ruptured LAD plaque and they stented this area, which ensures the stability of the plaque. The image on the left shows the LAD before intervention, and the red circled portion on the right indicates the stented region. This is not the case.
12.6), the rate of complete occlusion was 75.2% (91/121), ≥50% in-stent stenosis 7% (9/129), and retreatment 0.8% (1/129). Analysis included patients with unruptured wide-necked saccular aneurysms (not previously treated), measuring <12 mm along the ICA segments. Successful implantation was encountered in 99% (128/129) of the cases.
Cath lab was activated, and found a 95% proximal LAD occlusion which was stented. As Smith and Meyers explained in a 2020 article in EM News : “What should we do in the meantime while we are still stuck in the STEMI paradigm in daily practice? First, start using the terminology that allows our understanding to progress.
Successful drug-eluting stent placement opening up 95% mid RCA stenosis to 0% residual Nonobstructive left system disease. To add to this complexity ( as per My Comment in the August 22, 2020 post in Dr. Smith's ECG Blog ) — the ST-T wave appearance in repolarization variants may be dynamic ! Below the limit of detection.
Only 24 patients received intravenous thrombolytics (5.3%) and 47 had stent placement (10.4%). A total of 3 separate groups, low‐dose ticagrelor (45 mg or 60 mg twice a day), full‐dose ticagrelor (90 mg twice a day) and clopidogrel (75 mg daily) were created. Out of 445 patients, 288 were on aspirin 81 mg at time of discharge.
And finally, after placement of a stent in the LAD: Before and after: (Unfortunately, this resulted in the "jailing" of the septal branches behind the stent and probably some degree of plaque shift which is why they do not opacify well in the "after" shot. This was the cost of preventing infarction of the anterior wall.)
C ASE C onclusion : Timely cardiac cath was performed on today's patient — with successful reperfusion and stenting of his proximal LAD occlusion. = The importance of the new OMI ( vs the old STEMI ) Paradigm — See My Comment in the July 31, 2020 post in Dr. Smith's ECG Blog.
hours after that first diagnostic ECG) : Mid-LAD culprit lesion, 99% stenosis, no pre-intervention TIMI flow available, but described as "severe subtotal lesion", which was stented with reported TIMI 3 flow resulting. Another lesion in the proximal LAD with 80% stenosis was stented as well. Culprit lesion was reduced to 0% and stented.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. She also has a hx of paroxysmal atrial fibrillation and is on oral anticoagulant treatment. She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. The last echocardiography 12 months ago showed HFmrEF.
The culprit lesion was opened and stented. For those in search of brief review of the Cabrera Format for ECG recording — Please check out My Comment at the bottom of the page in the October 26, 2020 post in Dr. Smith's ECG Blog. The QoH now recognizes the OMI with mid confidence. Below is the post -PCI electrocardiogram.
It was opened and stented with resulting TIMI-3 (normal) flow. The stent to LCX is patent. not left main occlusion == MY Comment by K EN G RAUER, MD ( 1/16/2020 ): == I did not correctly identify the “culprit artery” in this case. OM1 is occluded and OM2 has 60% stenosis.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content