This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ). . = R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation.
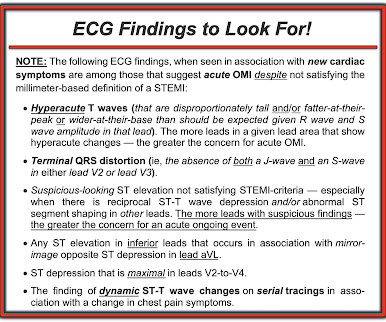
Figure-4: ECG findings to look for when your patient with new-onset cardiac symptoms does not manifest STEMI-criteria ST elevation on ECG. For more on this subject — SEE the September 3, 2020 post in Dr. Smith’s ECG Blog with 20-minute video talk by Dr. Meyers on The O MI M anifesto.
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Academic Emergency Medicine 27(S1): S220; May 2020. Cath attending is aware. It is a mass delusion.
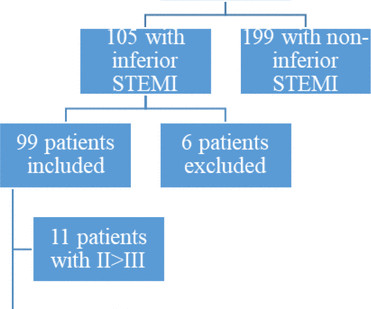
Background ST elevation myocardial infarction (STEMI) represents a cardiac emergency. Inferior STEMI represents a dilemma for cardiologists. Methods We performed a single-centre retrospective cohort analysis of all patients admitted to our hospital from 2008 to 2020 with a diagnosis of inferior STEMI.
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published.
This ECG was texted to me with the implied question "Is this a STEMI?": I responded that it is unlikely to be a STEMI. Septal STEMI often has ST depression in V5, V6, reciprocal to V1. Then combine with clinical presentation and low pretest probability 2 Saddleback STEMIs A Very Subtle LAD Occlusion.T-wave wave in V1??
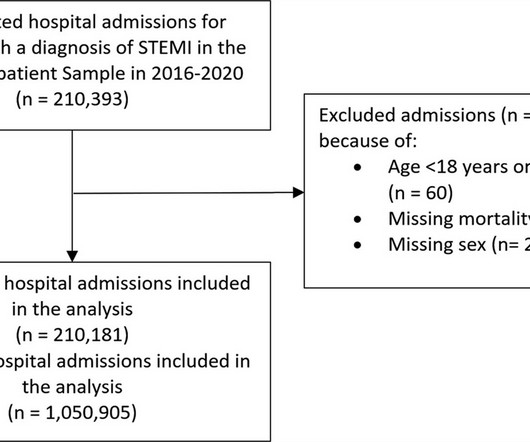
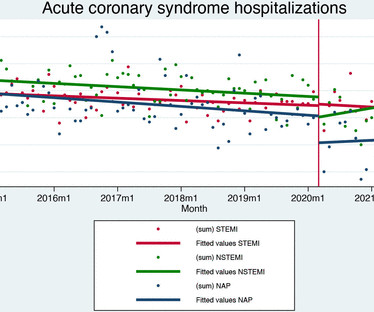
Background It is unclear how COVID-19 pandemic affected care and outcomes among patients who are diagnosed with ST-elevation myocardial infarction (STEMI) in the USA. Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2% reduction in admissions in 2020. reduction in admissions in 2020.
mmm ECG Blog #193 — Reviews the concept of why the term “OMI” ( = O cclusion-based MI ) should replace the more familiar term STEMI — and — reviews the basics on how to predict the " culprit " artery. The importance of the new OMI ( vs the old STEMI ) Paradigm — See My Comment in the July 31, 2020 post in Dr. Smith's ECG Blog.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Jason was very skeptical of STEMI. This also argues against STEMI. Look for old ECGs Do serial ECGs Do echocardiography == MY Comment by K EN G RAUER, MD ( 10/1/2020 ): == From time to time — it's helpful to "resurface" prior cases that convey timeless important lessons. He complained of 3 days of diarrhea and abdominal pain.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? This is the response he got: Interventionist: "No STEMI, no cath. After stabilizing the patient and recording more ECGs, he tried again: Interventionalist: "It isn't a STEMI." It is a STEMI equivalent. We don't know how many though.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
IMPRESSION: In this patient who presents with severe, new-onset CP — today's ECG is diagnostic of an extensive, ongoing antero-lateral STEMI. ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ).
Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. To Emphasize: The phenomenon of T-QRS-D is not needed in today's case to recognize the acute STEMI. The decision of whether to cath patients with a less definitive post-ROSC ECG is less clear.
If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management. What is the gold standard for ECG interpretation: patient outcome!!!
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern.
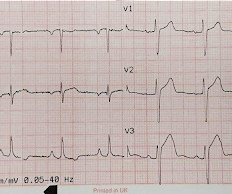
Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." He diagnosed anterior "STEMI" and activated the cath lab. 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
This was a machine read STEMI positive OMI. The meaning of this quote is that at times, something as obvious as the dramatic anterior lead ST elevation that we see in today's tracing is not the result of an acute LAD STEMI. His ECG is shown below. Pretty obvious anterior current of injury. What would you guess is the culprit artery?
ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ). R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation.
In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. In other words, the inferior "ST elevation" is due to the abnormal rhythm, and does not signify OMI or STEMI in any way. This situation has been named "Emery phenomenon." YOU TOO CAN HAVE THE PM Cardio AI BOT!!
These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ). ECG Blog #185 — Reviews the P s, Q s, 3 R Approach to Rhythm Interpretation.
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Learning Points: You cannot trust conventional algorithms even to find STEMI(+) OMI, even when they say "normal ECG." At this point — a STEMI was diagnosed, and cardiac cath with PCI was performed.
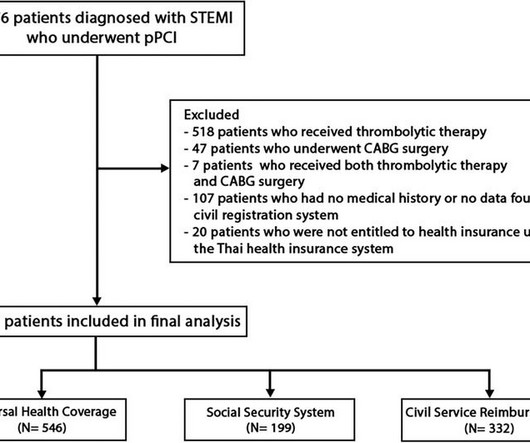
BackgroundIn Thailand, access to specific pharmaceuticals and medical devices for ST-elevation myocardial infarction (STEMI) patients is restricted within certain healthcare systems, leading to inequalities in the quality of medical care among different healthcare systems.
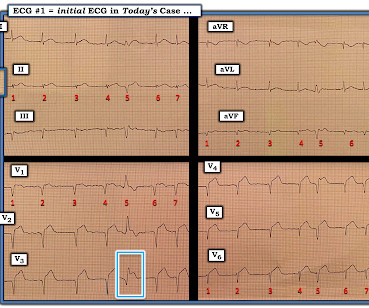
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS.
Data were fitted to segmented regression models with March 2020 as the breakpoint. Data on 21 001 patients were included (7057 ST-elevation myocardial infarction (STEMI), 7649 non-ST elevation myocardial infarction (NSTEMI) and 6295 unstable angina). to 2.1%, p=0.755) or in-hospital mortality (0.1%, (95% CI) –0.9%
P utting I t A ll T ogether : After correcting for LA-LL lead reversal — ECG # 1a shows sinus rhythm — LVH — and an acute infero-postero STEMI with acute RV involvement. PEARL # 3: In the absence of an anterior STEMI — acute inferior MI is the result of either acute RCA or LCx ( L eft C ircumfle x ) coronary occlusion.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. He wrote most of it and I (Smith) edited.
BOTTOM Line: The ECG in Figure-4 shows an extensive infero-postero-lateral STEMI. Working through a case of a regular WCT Rhythm in this 80-something woman — See My Comment in the May 5, 2020 post on Dr. Smith’s ECG Blog. Smith’s ECG Blog. ECG Blog #351 — Blog #285 — Blog 246 — Blog #80 — for examples of acute posterior OMI.
ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ). . = R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation.
ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ). . = R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al. Circulation. 2017;135(16):1490–3.
There is an obvious inferior posterior STEMI(+) OMI. Methods Retrospective study of consecutive inferior STEMI , comparing ECGs of patients with, to those without, RVMI, as determined by angiographic coronary occlusion proximal to the RV marginal branch. The February 11, 2020 post ( LA-RA reversal ). What is the atrial activity?
Background Despite advances in percutaneous coronary intervention (PCI) for ST segment elevation myocardial infarction (STEMI), in-hospital mortality remains a concern, highlighting the need for the identification of additional risk factors such as serum iron levels. μmol/L) and a control group (Fe ≥7.8 μmol/L).
— See My Comment at the bottom of the page in the October 14, 2020 post on Dr. Smith's ECG Blog. Acute OMI that wasn’t accepted by the Attending — See My Comment at the bottom of the page in the November 21, 2020 post on Dr. Smith’s ECG Blog.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. Large STEMI are approximately 30-80.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Day 12 ECG: FINAL DIAGNOSIS: "NSTEMI" Despite the fact that his day 4 ECG easily meets STEMI criteria, the patient is diagnosed as NSTEMI. Academic Emergency Medicine 27(S1): S220; May 2020.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
Figure-4: ECG findings to look for when your patient with new-onset cardiac symptoms does not manifest STEMI-criteria ST elevation on ECG. For more on this subject — SEE the September 3, 2020 post in Dr. Smith’s ECG Blog with 20-minute video talk by Dr. Meyers on The O MI M anifesto.
EKG from triage: Here is his previous ECG: Normal ST Elevation Resident's interpretation: Reperfusion pattern/Wellens' with biphasic T waves in V2 and V3, and in comparison to an EKG in 2020 this is new. Patient still not having chest pain however this is more concerning for OMI/STEMI. Labs ordered but not yet drawn. Aspirin given.
The history and associated deep anterior S waves (ie, the reciprocal of tall lateral lead R waves ) will suggest LVH rather than Precordial Swirl ( See ECG Blog #254 and My Comment at the bottom of the page in the February 6, 2020 and June 20, 2020 posts in Dr. Smith's ECG Blog ). ECG Blog #367 — for another example of acute LCx OMI.
For technical reasons — P waves are not well visible in this tracing — BUT — the P wave in lead I appears to be larger than the P wave in lead II , which is often a tip-off to LA-LL Reversal ( See My Comment in the November 19, 2020 and the May 24, 2022 posts in Dr. Smith's ECG Blog ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content