This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
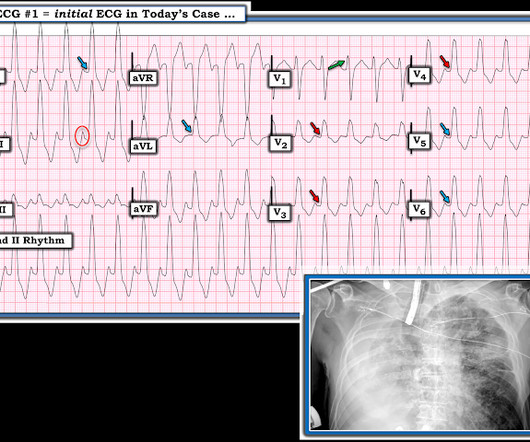
On the monitor patient had wide-complex tachycardia. Differential is ventricular tachycardia versus supraventricular tachycardia with aberrancy versus sinus tachycardia with a aberrancy. After the patient was stabilized with supportive care, the heart rate gradually slowed, confirming sinus tachycardia.
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
She had acute pulmonary edema on exam. On arrival, lung ultrasound confirmed pulmonary edema (B lines). In comparison to the previous study, 11/11/2020, there has been a significant interval deterioration of left ventricular systolic function (previous EF 80%), and there is a new large apical wall motion abnormality.
Multifocal Atrial Tachycardia 2. of all cases, and 62% of Veritas® misdiagnoses). == MY Comment , by K EN G RAUER, MD ( 1/5/2020 ): == This case illustrates a number of important teaching points. The rhythm is indeed irregularly irregular, so atrial fibrillation must be considered. Sinus with multifocal PACs 3. GET a 12-lead!
In the context of today's case — these P waves are diagnostic of RAE = P Pulmonale ( See ECG Blog #75 ) and almost certain associated pulmonary hypertension. Retrospectively — I interpret this 1:1 retrograde conduction as diagnostic of a reentry SVT rhythm as the etiology of the initial tachycardia.
Smith interpretation: This is highly likely to be due to extreme right heart strain and is nearly diagnostic of pulmonary embolism. It is of course pulmonary embolism. No d-dimer or CT pulmonary angiogram was done when they discovered that she had normal coronary arteries. What is the clear diagnosis and reason for arrest?
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( Hypoxic injury ( from pneumonia or other acute pulmonary complication ).
Smith comment: before reading anything else, this case screamed pulmonary embolism to me. I would do bedside ultrasound to look at the RV, look for B lines as a cause of hypoxia (which would support OMI, and argue against PE), and if any doubt persists, a rapid CT pulmonary angiogram. There is sinus tachycardia at ~100/minute.
My answer: "This is classic for PE, but it can also be present in any hypoxia due pulmonary hypoxic vasoconstriction and resulting acute pulmonary hypertension and acute right heart strain. Tachycardia (or nearly) 2. An ECG was texted to me (Smith) without any clinical information: What did I say? This is NOT Wellens.
The bedside echo showed a large RV (Does this mean there is a pulmonary embolism as the etiology?) When you suspect pulmonary embolism due to large RV on POCUS, always look for right axis deviation and a large R-wave in V1 because the large RV may be entirely due to chronic RVH, not acute PE. Here is his triage ECG: What do you think?
Further ultrasound showed no B-lines (no pulmonary edema). 23/WCC — 2/21/2020 ). 23/WCC — 2/21/2020 ). 23/WCC — 2/21/2020 ). 23/WCC — 2/21/2020 ). The heart rate is too fast for this poor filling. Preload must be increased and the heart rate slowed in order to allow more LV filling.
and the patient was converted to veno-venous (V-V) ECMO due to persistent pulmonary insufficiency. Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. medRxiv [Internet] 2020;Available from: [link] 8.
ECG Blog #65 — for an example of MAT in a patient with chronic pulmonary disease ( plus more on the differential diagnosis of MAT ). These cases provide insight to assessment for MAT: The January 5, 2020 post in Dr. Smith’s ECG Blog — for an example of MAT. ECG Blog #199 and ECG Blog #366 — for Review of M AT.
His prehospital ECG showed "inferior" ST depression and high voltage, with tachycardia. I suspected no OMI, that this could be due to LVH plus tachycardia. The estimated pulmonary artery systolic pressure is 29 mmHg + RA pressure. On arrival to the ED, the patient was diaphoretic, tachycardic. and had dilated pupils.
They include myocardial ischemia, acute pericarditis, pulmonary embolism, external compression due to mass over the right ventricular outflow tract region, and metabolic disorders like hyper or hypokalemia and hypercalcemia. 2020 Sep;31(9):2474-2483. J Cardiovasc Electrophysiol. Gourraud JB, Barc J, Thollet A, Le Marec H, Probst V.
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
AF patients received 4-step ablation composed of EIVOM, pulmonary vein isolation (PVI) and linear ablation. The primary composite endpoint was defined as recurrence of atrial tachycardia over 30 s.
Smith comments : Wide complex tachycardia. The differential diagnosis of WCT is: 1) Sinus tachycardia with "aberrancy" (in this case RBBB and LAFB), but there are no P-waves and the QRS morphology is not typical of simple RBBB/LAFB. Also, if the rate is constant, not wavering up and down, it is highly unlikely to be sinus tachycardia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content