This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundPlaque progression (PP) is critical between subclinical atherosclerosis and plaque rupture. Journal of the American Heart Association, Ahead of Print. Small dense lowdensity lipoprotein cholesterol (sdLDLC) is considered as the most atherogenic lipoprotein.
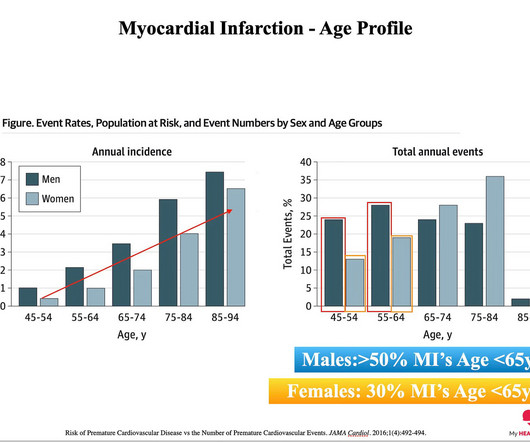
The reason: They were accumulating plaque in their coronary arteries much earlier than their peers. You can’t have a heart attack if you don’t have plaque in your coronary arteries. And plaque in your coronary arteries is the result of exposure to risk factors over time. The answer: Risk Factors. The answer.
We used carotid ultrasounds to detect plaque at baseline and follow‐up in 2006 to 2009 (median follow‐up=5.5 We identified incident CVD events through 2020 with a median follow‐up of 18.5 had incident plaque (109/1104 plaque‐free participants with baseline and follow‐up ultrasounds), 11.0% Approximately 2.8%
The breakthrough designation, according to the Milpitas, CA-based technology company, is for an indication to improve coronary luminal diameter, restore hemodynamic modulation, and reduce plaque progression in patients with symptomatic ischemic heart disease due to discrete de novo native coronary artery lesions. JACC 2020. of the U.S.
FFRCT, coronary plaque, etc). in 2020-2022, and 13.5% Cardiovascular AI’s falling share is partially due to a surge in AI products from new specialties (orthopedics, pathology, urology, ENT), but it’s mainly because non-cardiac radiology AI applications scored a whopping 544 clearances since 2020. since the start of 2023.
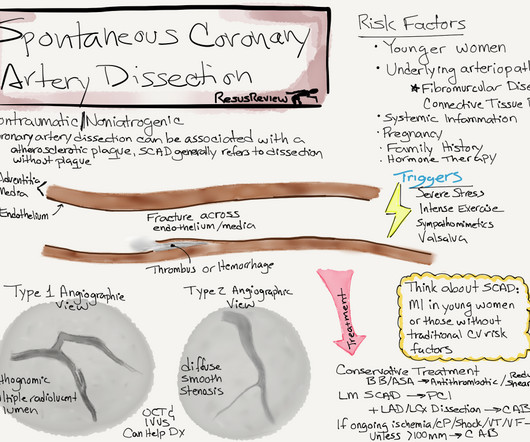
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. Thus, intracoronary imaging modalities are crucial in this setting. From Gue at al.
This has important clinical significance , as many successfully lysed STEMI patient might have minimal segments of dissection/deep plaque fissures. , Kim N Engl J Med 2020; 383:2358-2370 Next query What is the difference between plaque fissure and coronary arterial dissection? Is plaque fissure painful ?
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. It is not rare.
The incidence of no-reflow was higher in patients with attenuated plaque ≥5 mm in length as evaluated by intravascular ultrasound (IVUS).Objective:The The incidence of no-reflow was higher in patients with attenuated plaque ≥5 mm in length as evaluated by intravascular ultrasound (IVUS).Objective:The vs. 8.6%, p < 0.001).
If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA. Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus." They often cannot even be recognized as culprits, as fissured or ulcerated plaque. FFR can be useful.
There will be an award for the most cited national manuscript in 2022, considering the articles published in 2020 and 2021, for ABC Cardiol and IJCS journals; and the most accessed in 2022 for the ABC Imagem and ABC HF journals. Prizes awarded to the first author: a) Plaque for each awarded article. c) Credit of R$ 2,000.00
FFRCT, coronary plaque, echo AI, etc)… We’re using this broader definition of cardio AI through the rest of this story. Cardiovascular AI’s total share of H1 2024 AI clearances was the highest since 2020 (both 18%), after landing between 14% and 16% during the last three years.
EKG from triage: Here is his previous ECG: Normal ST Elevation Resident's interpretation: Reperfusion pattern/Wellens' with biphasic T waves in V2 and V3, and in comparison to an EKG in 2020 this is new. Angiography : --Culprit for the patient's unstable angina/Wellen syndrome is a ruptured plaque in the mid LAD. --As
To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! One of the most common is rupture of a non-obstructive plaque, with thrombus formation and OMI that spontaneously lyses and leaves a wide open artery. It can only be seen by IVUS.
To standardize (2), aspiration was to be initiated just before PTA balloon deflation during pre- and post-dilatation.Methods:From June 2020 to the present, CAS cases using the Filter protection device were enrolled and divided into two groups before and after the introduction of the POWER technique. Symptomatic stenosis (63.9%
Mild Plaque no angiographically significant obstructive coronary artery disease. In comparison to the previous study, 11/11/2020, there has been a significant interval deterioration of left ventricular systolic function (previous EF 80%), and there is a new large apical wall motion abnormality. I looks as if there has been reperfusion.
Ramus: There is a large caliber branching ramus intermediate LAD is a medium caliber vessel that extends to the apex and is noted to have diffuse mild to moderate plaque in the midsegment. Post Procedure TIMI III. D1 is a medium caliber vessel, distal diagonal branches are small in caliber Echocardiogram Normal LV cavity size and thickness.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
Reperfusion of OMI indicates at least partial thrombolysis of occluding thrombus, but still unstable plaque rupture, which can reocclude at any moment. For discussion of these cases — Please see My Comment at the bottom of the page in the June 20, 2020 post — the July 29, 2022 post — the August 15, 2022 post — and the September 30, 2022 post.
And finally, after placement of a stent in the LAD: Before and after: (Unfortunately, this resulted in the "jailing" of the septal branches behind the stent and probably some degree of plaque shift which is why they do not opacify well in the "after" shot. This was the cost of preventing infarction of the anterior wall.) ng/mL (ref.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
Therefore it means acute type 1 ACS plaque rupture with impeded flow and impending full occlusion until proven otherwise. Academic Emergency Medicine 27(S1): S220; May 2020. Then, the patients third ECG showed a very rare combination of de Winter T waves happening during LBBB.
Angiogram: Severe coronary artery calcification Moderate to severe distal small vessel disease mainly seen in RPL1, 2 Otherwise, Mild plaque, no angiographically significant obstructive coronary artery disease. IF interested in more on the topic of fragmentation — See My Comment in the January 31, 2020 post.
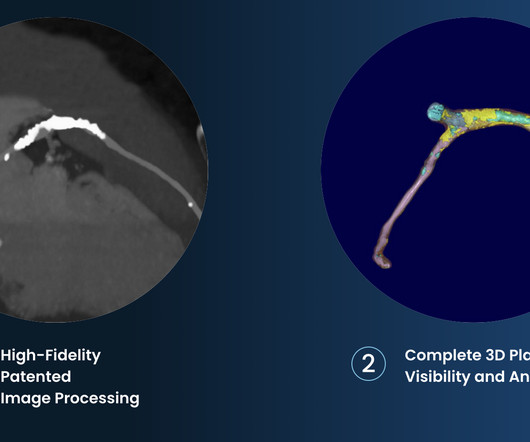
This registry will aim to provide world-wide physicians the most accurate information on coronary plaque to improve cardiovascular risk prediction and support the selection of patient-specific treatment,” said Dr. De Cecco. The ultimate goal is to positively impact cardiovascular health globally with a reduction in cardiovascular events."
She was treated medically for NonSTEMI, pending next day cath, which showed ulcerated plaque and a 60% thrombotic stenosis in the LAD distal to the first diagonal. A formal contrast echo was done at this point : Normal estimated left ventricular ejection fraction, 65%. Regional wall motion abnormality-distal septum and apex. It was stented.
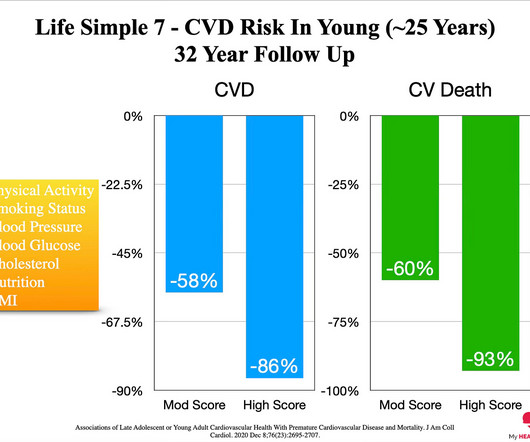
By the time you get to age 80, you will almost certainly have evidence of plaque in your coronary arteries - you will have heart disease. 2020 Dec 8;76(23):2695-2707. But first, let’s get some facts straight. Over a long enough time frame, pretty much everyone will get heart disease. Heart attacks do. J Am Coll Cardiol.
Recent evidence suggests that nonstenotic carotid plaque (nsCP) may be a substantial contributor to the risk for ESUS. Stroke, Ahead of Print. BACKGROUND:Many ischemic strokes are diagnosed as embolic strokes of undetermined source (ESUS).
There are multiple possible clinical situations that could account for diffuse subendocardial ischemia that is not due to ACS and plaque rupture. Figure-1: Reasons for the varied ECG presentation of acute LMain occlusion — excerpted from Dr. Smith’s 8/9/2019 post ( This Table from My Comment in the January 16, 2020 post ).
Heart disease is the presence of plaque or atherosclerosis in the coronary arteries. Over a long enough time horizon, pretty much everyone will develop a significant amount of plaque and have a heart attack. We have very strong evidence to support the idea that the more plaque you have, the greater your risk of a heart attack 1.
When we say heart disease, what we really mean is plaque in the artery wall. If you already have evidence of substantial plaque on a cardiac CT or have had a heart attack already, your future risk is significantly increased. Lipids and Lipoproteins in 2020. You just need to know how. This Is Known As Atherosclerosis.
Purpose To evaluate the association between osteoporosis and coronary calcification and coronary plaque burden in patients with atherosclerosis and coronary artery disease (CAD). The coronary artery calcium score (CACS) and total coronary plaque burden were quantified using the Agatston and modified Gensini scores, respectively.
people from the general population), coronary artery calcium scores (CACS) are higher, indicating more calcification and the presence of atherosclerotic plaques. Calcified plaques are known to be more stable and less prone to rupture and lead to a heart attack. When comparing athletes to control groups (i.e., hours per week).
A CTCA provides much more anatomical detail and can identify advanced plaque often missed by CT Coronary Artery Calcium Score scans alone. There are 3 types of coronary atherosclerosis visible on CTCA: Calcified Plaque - Easily Identified on both CT CAC & CTCA scans. Subscribe now How Often Does A CT CAC Scan Miss Plaque?
However, most adults will start to develop advanced plaque in their coronary arteries early in life. By age 66, more than half of all females will have evidence of advanced plaque in their coronary arteries, as seen on a CT calcium score. Coronary atherosclerosis, as evidenced by an abnormal CAC score, is a measure of advanced plaque.
Share Let’s first state our goal when we are in the business of ‘Heart Disease Prevention’: To delay the onset of coronary artery disease (atherosclerosis/plaque) that might rupture and cause a heart attack. And the less plaque you have, the lower the risk of a heart attack. And it’s also WAY more common.
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 7 Research has shown inflammation plays a significant role in the development of atherosclerosis and ASCVD,8-10 and even the formation of plaque.11 2020 Apr 21;141(16):e774].
Arteries generally narrow and occlude for one of two reasons: The progressive accumulation of plaque. A plaque ruptures, and a clot forms in the artery, thereby occluding it. There are the ‘garden variety’ heart attacks whereby a plaque ruptures in the coronary artery, called a spontaneous heart attack. N Engl J Med.
The cause of angina usually involves inadequate blood flow reaching the heart muscle because of significant narrowing of the artery due to plaque buildup. 2020 Apr 9;382(15):1395-1407. There are many ways it can present but this is the most common. But coronary stenting is not the only way to reduce symptoms of angina. N Engl J Med.
As an aside, the LCx OMI is a type 2 event, since it is due to supply-demand mismatch from thrombus, and not due to atherosclerotic plaque rupture or erosion). The November 10, 2020 post — for PTA. The October 17, 2020 post — for a 70-year old woman with " Artifactual VT ". The March 17, 2023 post — for PTA.
plaque disruption), the T waves still manifest markings of a previous state of suboptimal coronary flow that resolved: Type II supply-demand mismatch in the setting of extreme bradycardia. 2] Although the clinical context in today’s case does not fit these descriptors for Type I OMI (e.g. The Journal of Emergency Medicine, 51 (1), 1-8. [5]
Only after her troponin peaked at 500,000 ng/L did she get her angiogram, which showed a 100% left main occlusion due to ruptured plaque. Young people can suffer acute coronary occlusion, whether by typical atherosclerotic plaque rupture, or by coronary anomalies, coronary aneurysms, dissections, spasm, etc. Diagnostic of Massive OMI.
In 2020, 2.2 Inflammatory cytokines causing unstable plaques lead on to cardiovascular events [1]. Authors of the study under discussion [1] estimated that about 340,000 people died in 2020 from sugar sweetened beverages related type 2 diabetes and cardiovascular disease. of incident cases. million, contributing to 3.1%
Provocative testing is very helpful for this Coronary Thrombus with lysis (one must do optical coherence tomography or at least intravascular ultrasound to find thes non-obstructive plaques that ruptured. For more on the ECG diagnosis and consequences of acute RV MI Check out My Comment in July 19, 2020 post and the August 2, 2024 post).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content