This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
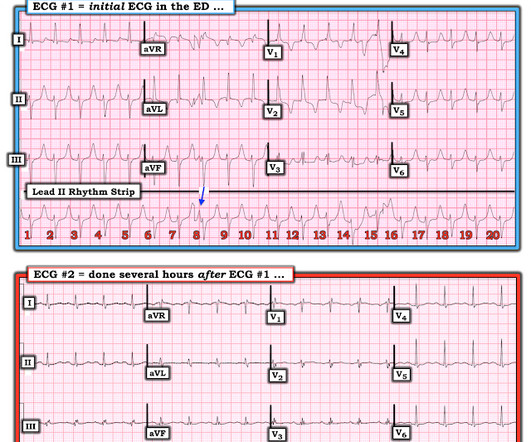
KEY Point: Although true that patients with longstanding, severe pulmonary disease may manifest a QRST complex in standard lead I with marked overall reduction in QRST amplitude ( See ECG Blog #65 — regarding Schamroth’s Sign ) — you should never normally see a completely flat line in any of the standard limb leads.
This suggests that there is pulmonary hypertension and thus possibly RVH. The estimated pulmonary artery systolic pressure is 31 mmHg + RA pressure. In a patient with RVH — the finding of a qR pattern has been closely correlated with pulmonary hypertension. Right atrial enlargement, severe. Severe tricuspid regurgitation. --The
My answer: "This is classic for PE, but it can also be present in any hypoxia due pulmonary hypoxic vasoconstriction and resulting acute pulmonary hypertension and acute right heart strain. The ECG of most patients with longstanding pulmonary disease show more r wave progression than I see in ECG #1. This is NOT Wellens.
The estimated pulmonary artery systolic pressure is 49 mmHg + RA pressure. It presents on the ECG as a long ST segment with resultant long QT == MY Comment by K EN G RAUER, MD ( 7/3/2020 ): == The patient in today’s case is a middle-aged woman who was brought to the ED following a motor vehicle accident.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










Let's personalize your content