This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Inflammatory pericarditis can occur in differential fashion. For example, the most common chronic pericarditis tuberculosis affects the fibrinous layer. Post MI pericarditis involves the epicardium. Diastolic Coronary Artery Compression in Constrictive Pericarditis. 2020 May 6;2(5):825-827. JACC Case Rep.
Here is his initial ED ECG: The R-wave in V4 extends to 33 mm, the computerized QTc is 372 ms The only available previous ECG is from one year ago, during the admission when he was diagnosed with pericarditis: 1 year ago ECG, with clinician and computer interpretatioin of pericarditis Normal 0 false false false EN-US X-NONE X-NONE What do you think?
It is easy to say pericarditis in such a case. young male no risk factors and ST-elevation in several leads) As Dr. Smith has emphasized many times you diagnose pericarditis at your patient's and your own peril. Version 1 was not trained to detect myo- or pericarditis. The above ECG was recorded. How did the Queen do?
Primary adverse events were defined as myocardial infarction, thromboembolism, transient ischemic attack, diaphragmatic paralysis, pneumothorax, heart block, pulmonary edema, vagal nerve injury, pericarditis, major vascular access complication or bleeding, death, stroke, or any other cerebrovascular accident. Epub 2020 Jan 19.
These latter findings are typical of pericarditis, but pericarditis never has reciprocal ST depression. Usually with pericarditis and myocarditis — hyperacute T waves (HATW) are not present. S mith : there is STE in lead III and reciprocal STD in aVL. This is OMI until proven otherwise. Sometimes — You have to be there.
Haven't you been taught that this favors pericarditis? Weren't you taught that concave morphology favors pericarditis? Expert ECG interpretation can often distinguish normal variant STE from OMI from pericarditis. Smith = “You diagnose acute pericarditis at your peril”. We will study this soon with our database.
She was diagnosed with pericarditis and spent one day in the hospital without events. Much more classic findings of pericarditis. Learning Points: Pericardial effusion is a key piece of information for the diagnosis and prognosis of pericarditis. Another ECG was performed, and this time was noted to be markedly abnormal.
It could also be due to pericarditis or myocarditis, but I always say that "you diagnose pericarditis at your peril." The clinical presentation is very suggestive of myo-pericarditis. But one should always remember that acute MI is a far more common pathology than myo- or pericarditis. Pericarditis? 13, 2019 Dr.
First, many on Twitter said "Pericarditis". This is NOT pericarditis, which virtually NEVER has ST depression any where except aVR. See our publication: ST depression in lead aVL differentiates inferior ST-elevation myocardial infarction from pericarditis There is STE in inferior leads, high lateral leads, and V4-V6.
Of course the patient was saddled with the erroneous "pericarditis" diagnosis after CTs ruled also ruled out PE and dissection. Serial ECGs remained unchanged. Echo showed normal EF and no wall motion abnormalities, and no pericardial effusion. But he did well. 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
Well, don't we see diffuse ST Elevation in Myo-pericarditis (with STD in aVR)? But it is very distinct from hyperkalemia (and anything else, including VT), and such confusion can only be due to lack of familiarity, because, if you look closely, its morpholgoy is very different from anything else. So this is STEMI, right? Which artery?
Pericarditis is rare — but myocarditis is not , so especially in this age group — more information is needed to quickly determine if this could be an acute MI, myocarditis, or none of the above. That said — acute MI does occur in younger patients.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." St depression in lead AVL differentiates inferior st-elevation myocardial infarction from pericarditis. link] Bischof, J. Worrall, C.,
In practice — It appears that electrical alternans is most often seen in association with regular SVT rhythms ( See the example in My Comment at the bottom of the page, in the September 7, 2020 post in Dr. Smith's ECG Blog ). Seeing it in this context suggests ( but does not prove ) the existence of an AP ( A ccessory P athway ).
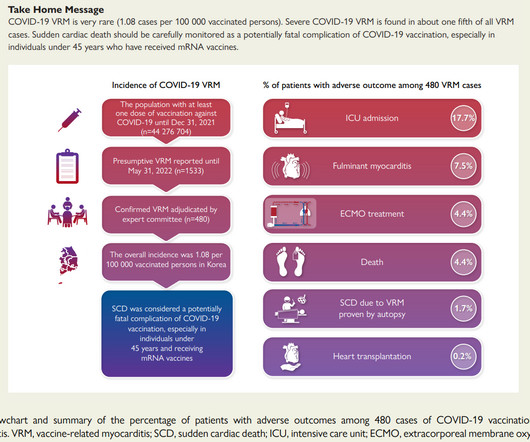
The KDCA also established a reporting system with a legal obligation for special adverse events including myocarditis and pericarditis after COVID-19 vaccination. Perhaps you decide vaccination is the right thing for you or your 13 year old after weighing the pros and cons.
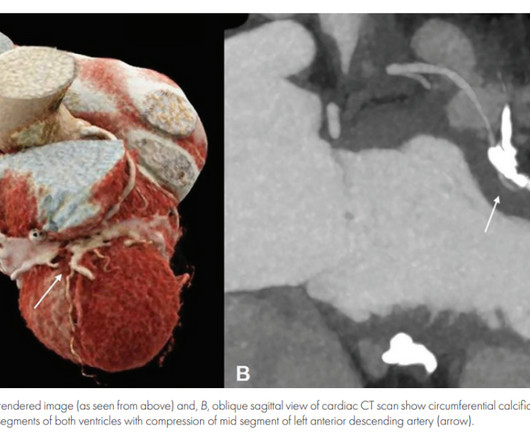
They include myocardial ischemia, acute pericarditis, pulmonary embolism, external compression due to mass over the right ventricular outflow tract region, and metabolic disorders like hyper or hypokalemia and hypercalcemia. 2020 Sep;31(9):2474-2483. J Cardiovasc Electrophysiol. Gourraud JB, Barc J, Thollet A, Le Marec H, Probst V.
As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. And a complication. == MY Comment by K EN G RAUER, MD ( 10/11/2020 ): == It cannot be stated any clearer than what Dr. Meyers states above. Is that normal?
The second most common cause of medical cardiac tamponade is acute idiopathic pericarditis. Less common etiologies include uremia, bacterial or tubercular pericarditis, chronic idiopathic pericarditis, hemorrhage, and other causes such as autoimmune diseases, radiation, myxedema, etc. What is ELECTRICAL ALTERNANS?
The "flu-like" illness suggests myo- or pericarditis, but that would be a diagnosis of exclusion. The November 10, 2020 post — for PTA. The October 17, 2020 post — for a 70-year old woman with " Artifactual VT ". Do not wait for the troponin; a lot of myocardium will be dead if you do. The case continues.
Assessment:" " Nonspecific ST elevation from V1-V4 , question of early repolarization versus pericarditis , question of acute current of injury and ? Pericarditis would be even more unlikely in someone without chest pain. Initial troponin came back negative." Sodium channel blockade effect from unidentified drug?" "In
Pericarditis? There is a literature on this subject ( GGF van der Schoot et al: Neth Heart J 28(6):301-308, 2020 — and — Egred et al — Postgrad Med 81(962): 741-745, 2005 — to name just 2 reports ). Chest Pain in a Male in his 20's; Inferior ST elevation: Inferior lead "early repol" diagnosed. Beware a negative Bedside ultrasound.
False Positive ST elevation in aVL Even when the story is obvious, with intractable pain, the STEMI paradigm can cause preventable delays Man in his 60's with very subtle ECG and pain not controlled with medical therapy Pericarditis vs. MI #2 See other "Quiz Posts": Quiz post - which of these, if any, are OMI? Will you activate the cath lab?
The case reports Case 1 involves a 26 year old man who developed pericarditis after the Pfizer vaccine. Pericarditis, an inflammation of the sac the heart lives in, developed about 7 days after the Pfizer vaccine. The diagnosis was made based on classic findings of inflammation on an electrocardiogram associated with acute chest pain.
It is relevant to note here that as a physician active clinically in both the inpatient and outpatient arenas, I am an eyewitness to the severe toll COVID19 took on my patients in the Spring or 2020. He has had COVID twice, first in September of 2020, and his second time in January of 2023. The pain resolved a few weeks later.
Though less prevalent in younger patients, occlusion MI may occur and requires the same early interventions as older patients. - - Pericarditis and myocarditis should be a diagnosis of exclusion. I've listed potential causes of acute pericarditis in My Comment at the bottom of the page in the June 11, 2022 post in Dr. Smith's ECG Blog.
Internat J Arrhyth 2020 Uesako H, Fukikawa H, Hashimoto S, et al. Prominent J waves and ventricular fibrillation caused by myocarditis and pericarditis after BNT162b2 mRNA COVID-19 vaccination. The relationship between J wave and ventricular tachycardia during Takotsubo cardiomyopathy.
The exception is with postinfarction pericarditis , in which a completed transmural infarct results in inflammation of the subepicardial myocardium and STE in the distribution of the infarct, and which results in increased STE and large upright T-waves. These findings together are more commonly seen with pericarditis.
Despite apparently hearing the above history together with two diagnostic ECGs and a troponin compatible with OMI, the cardiologist thought the ECG represented pericarditis and recommended echocardiogram. The emergency physician consulted cardiology. Several hours passed with no documentation as to the reason for delay.
The ‘prevaccination’ cohort comprised unvaccinated patients with CHD and matched controls with first-recorded SARS-CoV-2 infection between 1 March and 8 December 2020 (7805 cases, 27 620 controls). Compared with vaccinated controls, vaccinated patients with CHD remained at increased risk of hospitalisation (0.5%
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content