This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Opiates are associated with worse outcomes in Myocardial Infarction. Cath attending is aware.
They concluded, "Our findings increase confidence in the normal automated GE Marquette 12 SL ECG software interpretation to predict a benign outcome. Smith comment: this is a very stupid outcome measure) What if we use that methodology for the ECG above? Despite serial ECGs being "STEMI negative", the cath lab was activated.
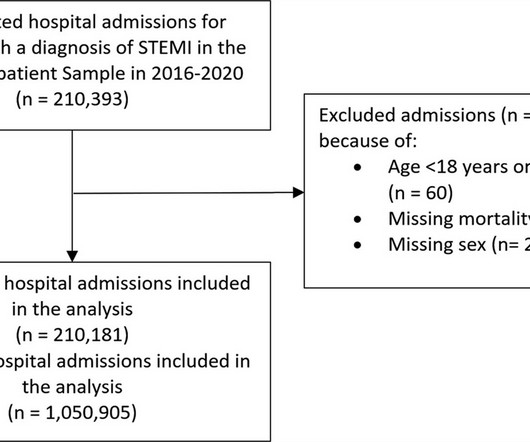
Background It is unclear how COVID-19 pandemic affected care and outcomes among patients who are diagnosed with ST-elevation myocardial infarction (STEMI) in the USA. Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2% reduction in admissions in 2020. reduction in admissions in 2020.
Jason was very skeptical of STEMI. This also argues against STEMI. What was the outcome? Outcome "I later found out that this is a patient who regularly calls paramedics to c/o chest pains and he had fooled many of them. He complained of 3 days of diarrhea and abdominal pain. What do you think? Jason, I agree.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? This is the response he got: Interventionist: "No STEMI, no cath. After stabilizing the patient and recording more ECGs, he tried again: Interventionalist: "It isn't a STEMI." It is a STEMI equivalent. We don't know how many though.
Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." He diagnosed anterior "STEMI" and activated the cath lab. 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
This was a machine read STEMI positive OMI. the investigators reviewed outcomes in 118 patients presenting with NSTEMI. The meaning of this quote is that at times, something as obvious as the dramatic anterior lead ST elevation that we see in today's tracing is not the result of an acute LAD STEMI. His ECG is shown below.
We present the cumulative percutaneous coronary intervention (PCI) data of all comers (stable angina and acute coronary syndromes [ACS]) who presented to Hadi Clinic between January 2018 and December 2020. A total of 567 patients underwent coronary catheterisation for the three-year period between January 2018 and December 2020.
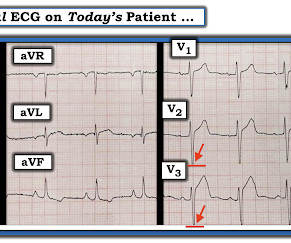
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Background Despite advances in percutaneous coronary intervention (PCI) for ST segment elevation myocardial infarction (STEMI), in-hospital mortality remains a concern, highlighting the need for the identification of additional risk factors such as serum iron levels. μmol/L) and a control group (Fe ≥7.8 μmol/L).
Frailty and CVD are often interrelated, affecting disease and treatment outcomes. Frailty is a syndrome of physiological decline, characterized by marked vulnerability to adverse health outcomes. Frailty is prevalent in adults with IHD requiring PCI. 10.23), intracranial hemorrhage (AOR = 4.65, 95% CI: 2.18-10.82),
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Circulation 2007 2. Khan et al.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Day 12 ECG: FINAL DIAGNOSIS: "NSTEMI" Despite the fact that his day 4 ECG easily meets STEMI criteria, the patient is diagnosed as NSTEMI. Long term outcome unknown but obviously bleak.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al. References: 1. Available from: [link] [link] 2.
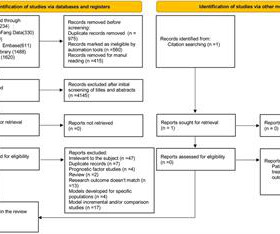
The purpose of this systematic review is to evaluate, describe, and compare existing models and analyze the factors that can predict outcomes. Methods We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 during the execution of this review.
There is an obvious inferior posterior STEMI(+) OMI. Methods Retrospective study of consecutive inferior STEMI , comparing ECGs of patients with, to those without, RVMI, as determined by angiographic coronary occlusion proximal to the RV marginal branch. The February 11, 2020 post ( LA-RA reversal ). What is the atrial activity?
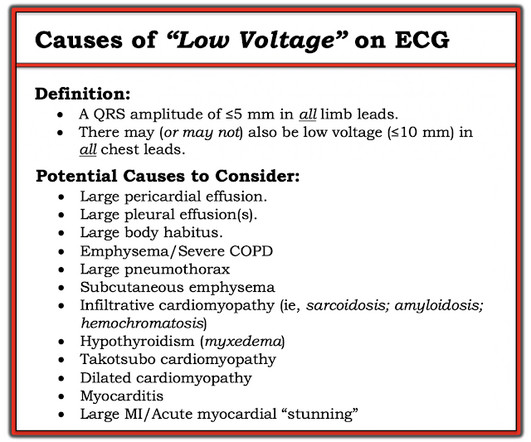
Outcome: 100% LAD Occlusion Here the Queen explains why: The dark blue tells us that she is looking especially at the QRS in V3 and the T-wave in V2 and V3. Not OMI, and we (Pendell and I) always take proportionality into account. So we taught the Queen on cases with very low voltage that were OMI.
EKG from triage: Here is his previous ECG: Normal ST Elevation Resident's interpretation: Reperfusion pattern/Wellens' with biphasic T waves in V2 and V3, and in comparison to an EKG in 2020 this is new. Patient still not having chest pain however this is more concerning for OMI/STEMI. Labs ordered but not yet drawn. Aspirin given.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
Non-randomized trials show better outcomes (neurologic survival) using this device; see this article in Resuscitation: Head and Thorax Elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival. Finally, head-up CPR (which was not used here), makes for better resuscitation.
Jason was very skeptical of STEMI. This also argues against STEMI. What was the outcome? Outcome "I later found out that this is a patient who regularly calls paramedics to c/o chest pains and he had fooled many of them. Look for old ECGs Do serial ECGs Do echocardiography June 17, 2016 Anterior STEMI?
Image from Ref 2 Egypt Heart J 72 , 28 (2020 Now, answer to the title question. Periprocedural and clinical outcomes of percutaneous coronary intervention of chronic total occlusions in patients with low- and mid-range ejection fractions. Egypt Heart J 72 , 28 (2020). Still it continue to be a smart move for many of us ?
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
Prehospital Conventional algorithm interpretation: ANTERIOR INFARCT, STEMI Transformed ECG by PM Cardio: PM Cardio AI Bot interpretation: OMI with High Confidence What do you think? Outcome : She was diagnosed with stress cardiomyopathy, though it is not entirely classic. She had acute pulmonary edema on exam.
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. As a result, this 45-year old man did not experince any delay in treatment — and a large diagonal branch of the LAD was stented with good outcome. To the uninitiated — this ECG may appear normal.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al. References: 1. Available from: [link] [link] 2.
Here is PM Cardio's Queen of Hearts interpretation (AI ECG interpretation trained by Meyers, Smith, and PM Cardio team using thousands of cases and their outcomes): The output number ranges from 0 to 1, with numbers closer to zero meaning likely NOT OMI, and numbers closer to 1 meaning OMI.
ECG read as: "Shows T wave inversions in the inferior leads and less than 1mm STE in V2, without STEMI criteria." Learning Points It takes dedicated learning and observation of outcomes and serial ECGs to learn how to distinguish subtle OMI patterns from OMI mimics like the cases above. All very very subtle. Aspirin was given.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). Yet this is rarely followed, and patient outcomes like this are the result once in a while.
Immediate and early percutaneous coronary intervention in very high-risk and high-risk Non-STEMI patients. Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. Unfortunately, they follow their own guidelines only 6% of the time!! Lupu L, et al. mg/dL, K 3.5 Abstract 556.
This can only be due to STEMI. There is new data showing better outcomes when bystander lesions (non-culprit) are stented. == MY Comment by K EN G RAUER, MD ( 8/28/2020 ): == Dr. Smith highlights a number of important lessons to be learned from today’s case. I said "activate the cath lab." Sotalol prolongs the QT 7.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Immediate versus delayed invasive intervention for non-stemi patients. Academic Emergency Medicine 27(S1): S220; May 2020.
A reliable study would keep track of all patients with shockable arrest and analyze the ones who were not enrolled to see their outcomes. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab.
Background Despite improvements in outcomes of ST elevation myocardial infarction (STEMI), ventricular septal rupture (VSR) remains a known complication, carrying high mortality. The contemporary incidence, mortality, and management of post-STEMI VSR remains unclear.
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease.
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." As the troponin T was 1521 ng/L (peak troponin T over 1000 ng/L is typical of STEMI) and still rising, no further troponins were measured. Unfortunately, no futher outcome is known (echo, survival, etc.) How does the Queen of Hearts do?
The provider contacted cardiology to discuss the case, but cardiology "didn't think it was a STEMI, didn't think he needed emergent cath." Could this outcome have been prevented with emergent cath? JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chest pain. Canto et al.
Practice putting the probe on the chest of someone with an obvious STEMI(+) OMI in order to look for regional wall motion abnormalities. Failure to consider the disease based on a patient's age will lead to missed diagnoses and worse outcomes. The subtle LAD OMI calculator, like any other diagnostic tool should not be followed blindly.
50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. 24 yo woman with chest pain: Is this STEMI? This is not "diffuse", this is simply anterior, lateral, and likely apical.
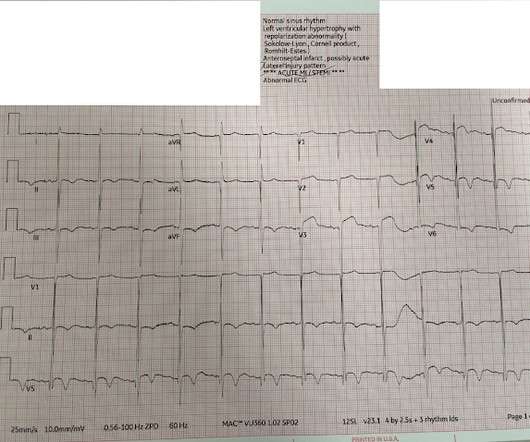
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. Of these, 48 met the primary outcome criteria of OMI. Figure-1: I've labeled today's ECG.
This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. 2020) If you are a regular reader of this blog this diagnosis will be easy for you, and you will manage this type of patient correctly with immediate revascularization.
He has a history of coronary artery disease and a STEMI two years prior that was treated with primary PCI. At the time of this initial ED ECG, his symptoms were improving ECG #1 on admission to the ED The patient was not seen quickly in the ED as it was a busy shift and the ECG did not meet STEMI criteria. The below ECG was recorded.
STEMI criteria are only 43% sensitive for OMI. Prevalence and outcome of patients with non-ST segment elevation myocardial infarction with occluded culprit artery - a systemic review and meta-analysis. Beware confusing the diagnosis of posterior STEMI by using posterior leads. Hung C-S, Chen Y-H, Huang C-C, et al.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content