This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Are you confident there is no ischemia? Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Is this: 1.
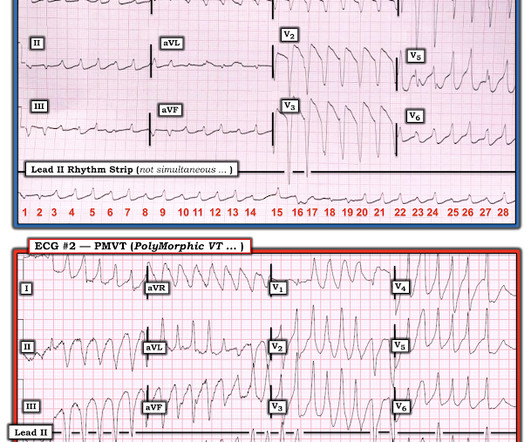
IMPRESSION: Given the presence of a wide tachycardia — with 2 distinct QRS morphologies, and no sign of P waves — a presumed diagnosis of B i D irectional Ventricular Tachycardia has to be made. Acute myocardial ischemia. See My Comment in the June 1, 2020 post in Dr. Smith's ECG Blog — for review of Pleomorphic VT.
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). During the next 24 hours, she experienced periods of complete AV block with a ventricular escape rhythm in the 20s.
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
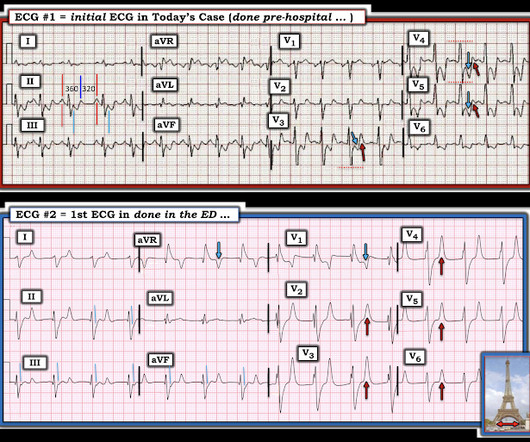
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
While the initial impression might not immediately suggest ventricular tachycardia (VT), a closer examination raises suspicion. Additionally, the qR morphology, particularly in a patient with right bundle branch block (RBBB) type wide QRS complex tachycardia (WQCT), lends further support for VT. What is the rhythm?
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. Analysis: there is a wide complex tachycardia. This was the interpretation I put into the system: WIDE COMPLEX TACHYCARDIA. It is regular.
This point is particularly relevant regarding ECG #2 — because sinus tachycardia is seen on this earlier ECG. In Figure-4 — I've reproduced from the above cited June 20, 2020 post my schematic illustration of the ST-T wave appearance that may be seen in one or more lateral leads for demonstrating LV "strain".
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). There is no definite evidence of acute ischemia. (ie, Some residual ischemia in the infarct border might still be present.
With normal EF the tachycardia is not compensatory. The same reciprocal relationship is seen in severe subendocardial ischemia, just with opposite vector direction where V1 can show ST elevation) Below you can find the 3D model of the heart and coronary vessels. And the patient has sinus tachycardia. ( HR about 90-100/min.
== MY Comment by K EN G RAUER, MD ( 6/1 /2020 ): == YOU are asked to interpret the ECG shown in Figure-1. When PMVT is associated with a long QT interval — the rhythm is then defined as Torsades de Pointes ( Please SEE My Comment at the bottom of the April 29, 2020 post in Dr. Smith’s ECG Blog ). Figure-1: The initial ECG in the ED.
In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) This is sinus tachycardia (rhythm) with complete heart block (AV node function) with ventricular escape rate just below 30. Never forget that sinus tachycardia is the scariest arrhythmia.
There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). This patient was having recurrent episodes of polymorphic ventricular tachycardia with an underlying long QT interval ( = Torsades des Pointes ). ECG #2 Interpretation of ECG #2: Underlying sinus rhythm.
MY Interpretation of Today's Initial ECG: I've labeled key findings in Figure-2 for today's initial ECG: The rhythm is sinus tachycardia at ~105/minute. The sinus tachycardia is a definite concern that something acute may be ongoing. Figure-2: I've labeled t he initial ECG. All intervals ( PR, QRS, QTc ) are normal.
ACUTE MI (I allowed Acute MI to be in the report because I knew there would be an elevated troponin from ischemia, which is the definition of acute MI -- but in this case it would most likely be a Type 2 MI from tachycardia) There is also LA-RA lead reversal. The February 11, 2020 post ( LA-RA reversal ).
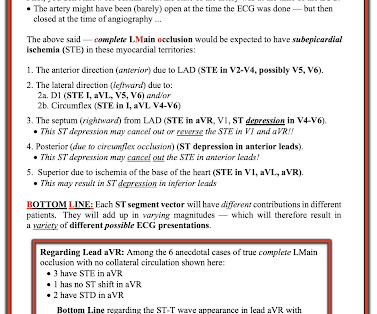
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] There is evolution from Wellens Pattern A to Pattern B, now inclusive of V6.
There is sinus tachycardia (do not be fooled into thinking this is VT or another wide complex tachycardia!) A repeat ECG was performed: An interesting mix of subendocardial ischemia pattern AND precordial swirl LAD OMI pattern. OMI and subendocardial ischemia patterns can both be present at the same time.
Here was the ECG: There is sinus tachycardia. Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia. This was sent by a reader. A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenic shock. and K was normal. This is "Shark Fin" morphology.
Here is the only prehospital 12-lead: Sinus tachycardia, somewhat wide QRS, Ischemia Here is the first ED ECG: What is the rhythm here? Medics found patient in PEA arrest. He was resuscitated into a perfusing rhythm. He went in and out of arrest until arrival at the ED.
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrial flutter with regular conduction. Now the patient is in sinus tachycardia. Her initial EKG is below. Adenosine worked.
Time 17 minutes Not much different One month earlier This is Left Bundle Branch Block (LBBB) without any sign of ischemia. If so, one would expect that the chest pain is diminishing or gone & that the culprit would be the LAD. It turns out that she spends much of her time in LBBB (see ECGs below) What is going on??? link] Shvilkin et al.
The terminology favored to describe these ECG findings is diffuse subendocardial ischemia ( See ECG Blog #271 — for more on diffuse subendocardial ischemia ). I discussed the findings of acute LMain occlusion further in My Comment in the January 16, 2020 post of Dr. Smith's ECG Blog. ECG Blog #316 — The patient died.
His prehospital ECG showed "inferior" ST depression and high voltage, with tachycardia. I suspected no OMI, that this could be due to LVH plus tachycardia. Conclusion: Type II MI probable due to hypoxia and tachycardia from resp arrest and amphetamine use. On arrival to the ED, the patient was diaphoretic, tachycardic.
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
First, we have a narrow-complex, regular tachycardia, with a rate of about 135-140. This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrial flutter. Tachycardia and ST Elevation. She was discharged home. Christmas Eve Special Gift!!
The ECG there reportedly showed an irregular tachycardia, and the patient was immediately referred to the emergency room. Here is her ECG on arrival: There is a wide complex tachycardia that is irregularly irregular (this is difficult to determine at these very high rates). Vitals were within normal limits other than heart rate.
Given the rapid rate of the tachycardia and the amorphous shape of the QRS — the decision was made to sedate the patient and cardiovert. This phenomenon may sometimes be seen following an episode of a sustained tachycardia — in which marked ST-T wave abnormalities not due to infarction may be seen for a period of hours, or even days!
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. JAMA Cardiol [Internet] 2020;Available from: [link] 4. JAMA Cardiol [Internet] 2020;Available from: [link] 5. Guo T, Fan Y, Chen M, et al.
Whether these EKGs show myocarditis, a normal variant, or something else, they are overall not typical of transmural ischemia of the anterior or high lateral walls. He had multiple episodes of bradycardia and nonsustained ventricular tachycardia. The patient had none of these conditions. Patient 1 remained in the hospital overnight.
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
They include myocardial ischemia, acute pericarditis, pulmonary embolism, external compression due to mass over the right ventricular outflow tract region, and metabolic disorders like hyper or hypokalemia and hypercalcemia. 2020 Sep;31(9):2474-2483. J Cardiovasc Electrophysiol. Gourraud JB, Barc J, Thollet A, Le Marec H, Probst V.
After initiating treatment for hyperkalemia, repeat ECG showed resolution of Brugada pattern: The ECG shows sinus tachycardia. A Very Wide Complex Tachycardia. These include ( among others ) — acute febrile illness — variations in autonomic tone — hypothermia — ischemia/infarction/cardiac arrest — and Hyperkalemia.
3 of the 4 have similarly bizarre PVCs. == MY Comment by K EN G RAUER, MD ( 4/29/2020 ): == Cardiac Arrest with Bizarre PVCs/Torsades de Pointes: Intriguing case with many interesting features. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia.
The flutter waves can conceal or mimic ischemic repolarization findings, but here I don't see any obvious findings of OMI or subendocardial ischemia. The rhythm in ECG #1 is not Sinus Tachycardia — because there is no upright P wave in lead II. The rhythm is 2:1 atrial flutter. I doubt that the rhythm is a reentry SVT.
Prior ECG available on file from 2 months before: We do not know the clinical events happening during this ECG, but there is borderline tachycardia, PVCs, and likely some evidence of subendocardial ischemia with small STDs maximal in V5-6/II, slight reciprocal STE in aVR. Notice the normal precordial T waves.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. She was ventilated by bag-valve-mask by EMS on arrival and was quickly intubated with etomidate and succinylcholine. A rectal temperature was obtained which read 107.9
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. There is no evidence of infarction or ischemia. An ECG was recorded: This shows a regular narrow complex tachycardia at a rate of about 160. There are nonspecific ST-T abnormalities. This seems to me to be very unlikely.
Occurrence of “J Waves” in 12-Lead ECG as a Marker of Acute Ischemia and Their Cellular Basis. The relationship between J wave and ventricular tachycardia during Takotsubo cardiomyopathy. Internat J Arrhyth 2020 Uesako H, Fukikawa H, Hashimoto S, et al. Acad Emerg Med 1999 Rituparna S, Suresh S, Chandrashekhar M, et al.
It is a wide complex regular tachycardia at a rate of 120. Is it ventricular tachycardia? I fear that many learners would also not easily recognize where the QRS actually ends, and I fear that some may think that this is ventricular tachycardia due to inability to distinguish QRS from ST segment. The ST Elevation is NOT typical.
T wave inversion as seen in ECG #2 is not uncommon following a sustained tachyarrhythmia ( sometimes called a "Memory Effect" or "post-tachycardia" syndrome ). In most cases when not due to a new infarction this post-tachycardia T wave inversion resolves over the ensuing hours ( and almost alwlays within 1-2 days ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content