This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This suggests further severe ischemia. MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. And yet the arteries remain open.
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia.
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. Ischemia can be disguised by a wide escape rhythm, which decreases the sensitivity of ECG.
Time 17 minutes Not much different One month earlier This is Left Bundle Branch Block (LBBB) without any sign of ischemia. Ramus: There is a large caliber branching ramus intermediate LAD is a medium caliber vessel that extends to the apex and is noted to have diffuse mild to moderate plaque in the midsegment. Post Procedure TIMI III.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m. ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! One of the most common is rupture of a non-obstructive plaque, with thrombus formation and OMI that spontaneously lyses and leaves a wide open artery. It can only be seen by IVUS.
Is this Acute Ischemia? Reperfusion of OMI indicates at least partial thrombolysis of occluding thrombus, but still unstable plaque rupture, which can reocclude at any moment. No formal echo was done, and EF was normal on ventriculogram during cath, with no obvious wall motion abnormalities. More on LVH. LVH with anterior ST Elevation.
This registry will aim to provide world-wide physicians the most accurate information on coronary plaque to improve cardiovascular risk prediction and support the selection of patient-specific treatment,” said Dr. De Cecco. The ultimate goal is to positively impact cardiovascular health globally with a reduction in cardiovascular events."
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
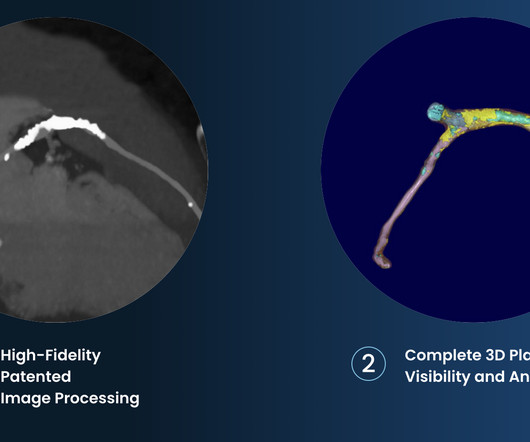
A CTCA provides much more anatomical detail and can identify advanced plaque often missed by CT Coronary Artery Calcium Score scans alone. There are 3 types of coronary atherosclerosis visible on CTCA: Calcified Plaque - Easily Identified on both CT CAC & CTCA scans. Subscribe now How Often Does A CT CAC Scan Miss Plaque?
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 7 Research has shown inflammation plays a significant role in the development of atherosclerosis and ASCVD,8-10 and even the formation of plaque.11 2020 Apr 21;141(16):e774].
Arteries generally narrow and occlude for one of two reasons: The progressive accumulation of plaque. A plaque ruptures, and a clot forms in the artery, thereby occluding it. There are the ‘garden variety’ heart attacks whereby a plaque ruptures in the coronary artery, called a spontaneous heart attack. N Engl J Med.
The cause of angina usually involves inadequate blood flow reaching the heart muscle because of significant narrowing of the artery due to plaque buildup. Subscribe now 1 ISCHEMIA Research Group. 2020 Apr 9;382(15):1395-1407. There are many ways it can present but this is the most common. N Engl J Med. 2 ORBITA investigators.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Lead V2 shows RR’ QRS configuration, and although ST depression is otherwise expected here, the discordance is a bit excessive. 5] Isnard, R.
Only after her troponin peaked at 500,000 ng/L did she get her angiogram, which showed a 100% left main occlusion due to ruptured plaque. Young people can suffer acute coronary occlusion, whether by typical atherosclerotic plaque rupture, or by coronary anomalies, coronary aneurysms, dissections, spasm, etc. Diagnostic of Massive OMI.
Influenza-like illness can also trigger plaque rupture. McLaren : The inferior T wave inversion suggests either reperfusion (if resolved symptoms) or subacute refractory ischemia and from the previous description of pain refractory to nitro it is likely the latter.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content