This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
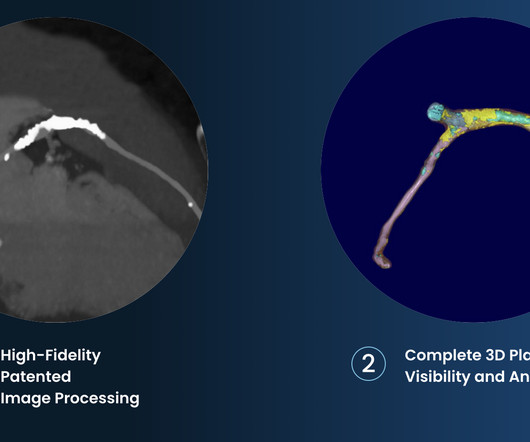
The company is also pursuing an indication for non-invasive measurement of fractional flow reserve (FFR CT ), uniquely derived from its plaque algorithm, to measure coronary blockages and the extent of ischemia. 2017 23, April 2020; Available from: [link]. Cardiovasc. 6 (3) (2019).
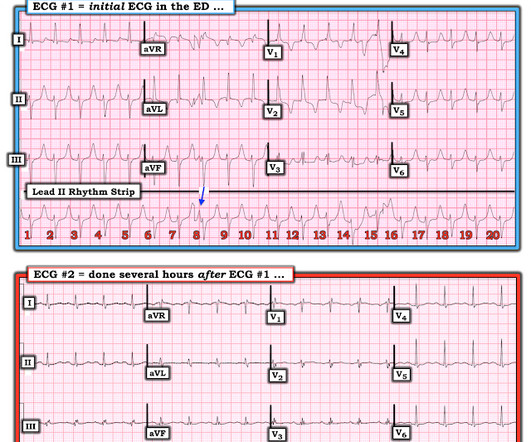
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy? How can you better assess the ST segments?
In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) The atrial rate is around 120 beats per minute, which indicates high adrenergic state and physiologic distress! I interpret tracings systematically in "real time" ( including my assessment for acute ischemia ).
Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). The physiologic reason for this — is thought to be the result of momentarily increased circulation from mechanical contraction arising from the "sandwiched in" QRS complex. The QRS complex in ECG #1 is wide.
We wish, our understanding about cardiac contractile physiology is deep and nearly complete. 2020) The un-disputable fact is ischemic DCM has a target to treat, though it is termed as cardiomyopathy. The simple reason could be we can address the ischemia a potential arrhythmic target by some form of revascularization in IDCM.
Either could be a result of myocardial contusion There is some minimal ST depression -- this could represent ischemia What else is there that could use therapy immediately? Regarding the RHYTHM in ECG #1: I’ve previously reviewed sequential ECG changes of Hyperkalemia ( For Review — SEE My Comment at the bottom of the January 26, 2020 post).
The fact that the heart rate is normal rules out demand side ischemia as well. Interpretation of T-wave inversion in physiological and pathological conditions: Current state and future perspectives. 2020 Aug;43(8):827-833. Epub 2020 Apr 7. This almost rules out an ACS or even a CCS. Reference 1. Clin Cardiol.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










Let's personalize your content