This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
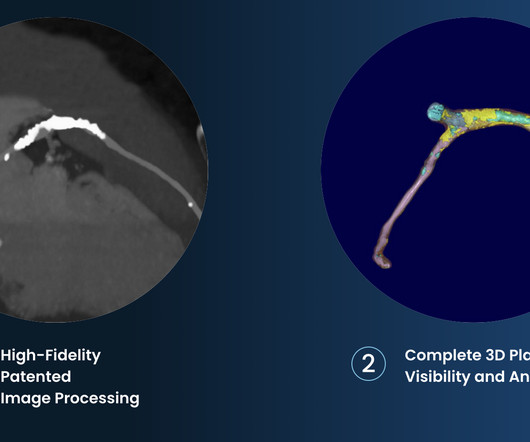
Cardiovascular disease is the most common cause of death and disability globally, largely driven by myocardialinfarction and ischemic stroke caused by atherosclerosis (plaque build-up in the arteries). 2017 23, April 2020; Available from: [link]. Cardiovasc. 6 (3) (2019).
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. The ECG is diagnostic of occlusion myocardialinfarction (OMI).
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m. ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
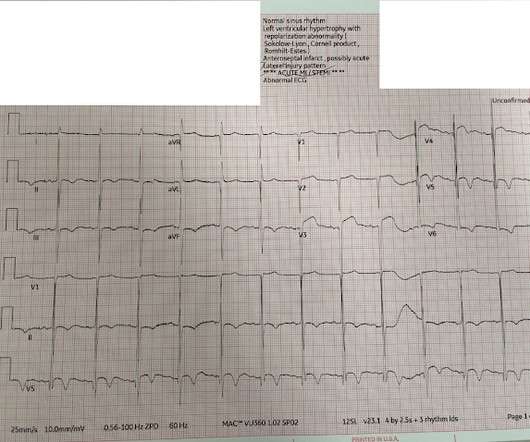
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. Nevertheless, the clinical situation made other etiologies unlikely. NTG drip started.
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia. Eur J Emerg Med.
There is probably a trickle of flow which is why there is both subendocardial ischemia (ST depression) and early subepicardial ischemia (hyperacute T-waves). Opiates are associated with worse outcomes in MyocardialInfarction. Academic Emergency Medicine 27(S1): S220; May 2020. Abstract 556.
5] Back to the case The patient had serial ECGs over the next hour with no significant change: The first troponin came back at 1,400 ng/L (normal <26 in males and <16 in females), confirming MI – and the patient’s refractory ischemia indicated this was an Occlusion MI. Clin Cardiol 2022 4. Herman, Meyers, Smith et al.
His father and brother both died of myocardialinfarction at ages 61 and 45, respectively. There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1]
The primary endpoint of this study was major adverse cardiovascular and cerebrovascular events (MACCEs) that included all-cause mortality, non-fatal myocardialinfarction, non-fatal ischemic stroke, and ischemia-driven revascularization.Results:The average age of the study participants was 59.55 ± 10.98
Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). There is no definite evidence of acute ischemia. (ie, Some residual ischemia in the infarct border might still be present.
This suggests further severe ischemia. associated typical MyocardialInfarction therapies such as statins and ACE inhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. Downstream vasospasm?
--The STD in V2-V6 might be interpreted as subendocardial ischemia, but with the inferior STE, it is far more likely to represent posterior OMI. In subendocardial ischemia, cath lab is indicated if the pain persists in spite of medical therapy (aspirin, anticoagulant, IV nitro). At 100 minutes, the above ECG was recorded.
The pain will resolve and you will think the ischemia is gone when it is only hidden ! Comparative early and late outcomes after primary percutaneous coronary intervention in st-segment elevation and Non–St-segment elevation acute myocardialinfarction (from the Cadillac trial). & Griffin, J. link] Lee, T. Weisberg, M.,
2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. The absence of STE in V7-V9 is often due to resolution of ischemia, as seen by resolution of ST depression in V7-V9. V5-V6) of any amplitude, is specific for Occlusion MyocardialInfarction (vs.
Triage ECG (no prior for comparison): Computer algorithm read: "Sinus rhythm, low voltage QRS, inferior myocardialinfarction, probably old." Smith : the profound persistent STE suggests either persistent occlusion or " no reflow " with persistent downstream ischemia. Academic Emergency Medicine 27(S1): S220; May 2020.
My interpretation was: RBBB with hyperacute T-waves in V4-V6 that are all but diagnostic of LAD occlusion vs. post ROSC ischemia. For more on the application of this Trace-down; Copy-over technique with Shark Fin ST segment deviations — See My Comment in the May 19, 2020 post in Dr. Smith's ECG Blog.
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. For this reason, some argue that it should not be measured in patients unless acute myocardialinfarction is on the differential diagnosis.
But ECGs interpretation is often conflated with clinical assessment, so if patients don’t present with chest pain the ischemic changes are not seen or are attributed to something other than ischemia. Clinical characteristics of dialysis patients with acute myocardialinfarction in the United States. Circulation 2007 2.
3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heart attack or myocardialinfarction (MI), stroke, and cardiovascular (CV) death.4 2020 Jan 28;141(4):e60] [published correction appears in Circulation. 2020 Apr 21;141(16):e774]. 4 In the U.S. 12 Colchicine, 0.5
Am J Emerg Med 2020 3. ST-elevation myocardialinfarction after pharmacologic persantine stress test in a patient with Wellens’ syndrome. Single High-Sensitivity Cardiac Troponin I to Rule Out Acute MyocardialInfarction. Was this objective evidence of inducible ischemia accompanied by chest pain?
Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chest pain for the ischemia and potential syncope for brugada. Ischemia/infarction. It helps a little bit.
I do not think this ECG is by itself diagnostic of OMI (full thickness, subepicardial ischemia ), b ut comparison to a previous might reveal this ECG as diagnostic of OMI. Association between opioid analgesia and delays to cardiac catheterization of patients with occlusion MyocardialInfarctions. Abstract 556.
Does this mean that the ST depression in V3 represents "anterior" subendocardial ischemia, and not posterior OMI? This is most consistent with ischemia/infarction in the distribution of the left circumflex coronary artery. V5-V6) of any amplitude, is specific for Occlusion MyocardialInfarction (vs.
This is a case written by Dan Lee (One of our fantastic Hennepin Residents, class of 2020 ) edits by Smith A 60 something-year-old man with a history of ESRD, LVH and prior CABG presented after an episode of hypotension during his hemodialysis, run followed by a syncopal episode which caused his run to be terminated early. What can we learn?
The ECG is diagnostic of LAD occlusion (or even left main occlusion possibly), with the classic pattern of RBBB and LAFB with huge concordant STE in V1-V2, I, and aVL, with reciprocal depression in most other leads (and/or a component of subendocardial ischemia pattern). This is "shark fin" morphology. Code STEMI was activated. Eur Heart J.
2 Coronary CT Angiography and 5-Year Risk of MyocardialInfarction. 2020 Jan 14;41(3):407-477. 5 ISCHEMIA Research Group. 2020 Jan 14;41(3):407-477. 5 ISCHEMIA Research Group. 2020 Apr 9;382(15):1395-1407. Medicine (Baltimore). 2022 Sep 16;101(37):e30583. N Engl J Med. 2018 Sep 6;379(10):924-933.
In the STEMI/NSTEMI dichotomy, NSTEMI is supposed to mean non-occlusive myocardialinfarction, but this patient had transient Occlusion MI that was at risk for re-occlusion (like ‘transient STEMI’). Impact of total occluson of culprit artery in acute non-ST elevation myocardialinfarction: a systemic review and meta-analysis.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Comparison of the QRS complex, ST-segment, and T-wave among patients with left bundle branch block with and without acute myocardialinfarction.
Angiogram: Culprit for the patient's inferior ECG changes and non-ST elevation myocardialinfarction is a 100% acute thrombotic occlusion of the proximal RCA. Traditionally , Occlusion MI (OMI) myocardialinfarctions that are not STEMI are called NonSTEMI. They have large infarcts and high mortality.
This proves that the first one was, surprisingly, due to ischemia!! High-Sensitivity Cardiac Troponin Concentrations at Presentation in Patients With ST-Segment Elevation MyocardialInfarction. 1] Wereski, R., Chapman, A. Gray, A., & & Mills, N. JAMA Cardiology , 5 (11), 1302–1304.
Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients With MyocardialInfarction With Nonobstructive Coronary Artery Disease. An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! Lindahl et al.
Here is his ECG: There is no clear evidence of OMI or ischemia. A 40-something male with no previous cardiac disease presented with chest pain. There is a tiny amount of STE in aVL, but it is NOT in the context of a tiny R-wave. There is a tiny amount of STD in lead III, with some non-specific T-wave flattening. Cath lab was activated.
Clinical questions : Is this an occlusion myocardialinfarction and does the patient need the cath lab? Occurrence of “J Waves” in 12-Lead ECG as a Marker of Acute Ischemia and Their Cellular Basis. Internat J Arrhyth 2020 Uesako H, Fukikawa H, Hashimoto S, et al. Pacing Clin Electrophysiol.
ECG #3 is easily recognized as OMI and the AI model recommends immediate revascularization The patient in today's case received suboptimal care and suffered a substantial myocardialinfarction. This case highlights how T-waves are very important in the assessment of ischemia and dynamic changes in acute coronary syndrome.
Case A 76 year old man with chronic hypertension but no history of coronary disease or myocardialinfarction presented to the ED with chest pain at 2343. His triage EKG is shown below: There is left bundle branch block, so the EKG must be evaluated for ischemia by Smith-modified Sgarbossa criteria.
of patients with anterior myocardialinfarction ( 1 ). Tall precordial T waves with depressed ST take-off: an early sign of acute myocardialinfarction? This typically occurs in the setting of a rapidly reperfused coronary artery following a myocardialinfarction. Transient ischemia may lead to "stunning".
It could also, given a different clinical context be compatible with a subacute myocardialinfarction complicated by post infarct regional pericarditis. Due to the atypical and vague symptoms, the myocardialinfarct was not initially diagnosed. At presentation he had a history of dyspnea for 6 days.
Prevalence and outcome of patients with non-ST segment elevation myocardialinfarction with occluded culprit artery - a systemic review and meta-analysis. Despite no posterior ST elevation there is still anterior ST depression, and an enlarging R in V2 wave from posterior infarction. Hung C-S, Chen Y-H, Huang C-C, et al.
Puskarich Abstract Objectives Data suggest patients suffering acute coronary occlusion myocardialinfarction (OMI) benefit from prompt primary percutaneous intervention (PPCI). This link takes you to My Comment in the June 20, 2020 post in which I review a user-friendly approach to ECG recognition of LVH and "Strain".
Compared to TTE from 7/3/24: the anterior regional wall motion abnormality is new and is consistent with ischemia/infarction in the LAD territory == MY Comment , by K EN G RAUER, MD ( 11/20 /2024 ): == There are several insightful aspects of today's case. The November 10, 2020 post — for PTA. The March 17, 2023 post — for PTA.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content