This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
For more on this subject — SEE the September 3, 2020 post in Dr. Smith’s ECG Blog with 20-minute video talk by Dr. Meyers on The O MI M anifesto. ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ).
ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ). ECG Blog #271 — Reviews determination of the ST segment baseline ( with discussion of the entity of diffuse Subendocardial Ischemia).
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
BackgroundDelayed cerebral ischemia represents a significant contributor to death and disability following aneurysmal subarachnoid hemorrhage. Journal of the American Heart Association, Ahead of Print. Our analysis included 102 eligible studies.
The August 22, 2020 post in Dr. Smith's ECG Blog — which illustrates another case of dynamic ST-T wave changes that resulted from a repolarization variant. Smith's ECG Blog ( Please scroll down to the bottom of the page to see My Comment ). This case is remarkable for the d ynamic S T - T w ave c hanges that are seen.
Acute myocardial ischemia. See My Comment in the June 1, 2020 post in Dr. Smith's ECG Blog — for review of Pleomorphic VT. As reviewed by Almarzuqi et al ( Vasc Health Risk Mgmt 18:397-406, 2022 ) — Potential Causes of Bidirectional VT include: Digitalis toxicity. CPVT ( Catecholaminergic PolyMorphic VT ). Cardiac Sarcoidosis.
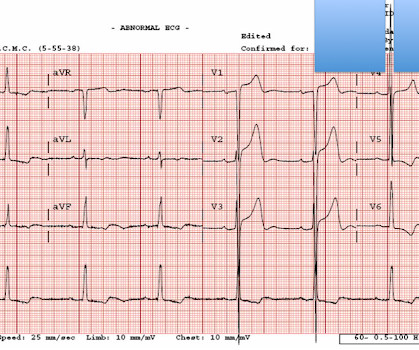
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). There is STE in aVR. Thus, there is high lateral OMI with diffuse ST depression. Moreover, left main occlusion often presents near death.
The ECG does not show any definite signs of ischemia. IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ).
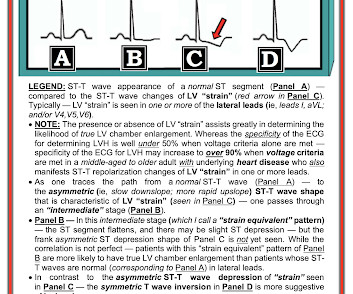
My written interpretation on a tracing such as this one would read, "Marked LVH and 'strain' and/or ischemia — with need for clinical correlation." BOTTOM LINE: ECG changes of LV "strain" and/or ischemia that we see on today's initial ECG — were not present 9 years earlier. Please see ECG Blog #73 for additional details ).
As a result, the ST elevation ( with especially tall, peaked T wave in lead V2) — is not indication of acute ischemia. As suggested by Figure-4 below in the ADDENDUM — assessment of the ST-T waves in leads V2,V3 and V5,V6 — is consistent with ischemia and / or LV "strain".
The history and associated deep anterior S waves (ie, the reciprocal of tall lateral lead R waves ) will suggest LVH rather than Precordial Swirl ( See ECG Blog #254 and My Comment at the bottom of the page in the February 6, 2020 and June 20, 2020 posts in Dr. Smith's ECG Blog ). Cardiol 27:674-677, 2004 ).
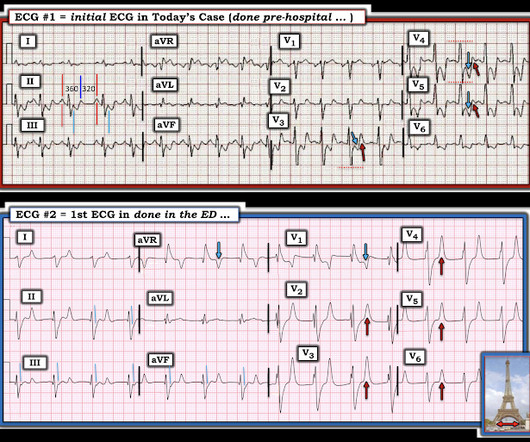
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. Nevertheless, the clinical situation made other etiologies unlikely.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. Remember that the RV is the most anterior chamber. Here is a transverse image of a CT showing this. A few clues that might have suggested this are: There is marked STE in V1.
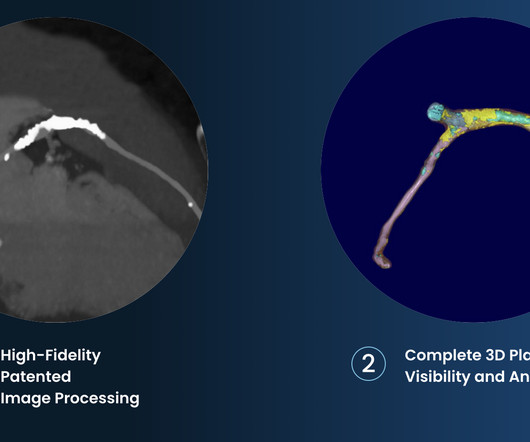
The company is also pursuing an indication for non-invasive measurement of fractional flow reserve (FFR CT ), uniquely derived from its plaque algorithm, to measure coronary blockages and the extent of ischemia. 2017 23, April 2020; Available from: [link]. Cardiovasc. 6 (3) (2019).
In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) I interpret tracings systematically in "real time" ( including my assessment for acute ischemia ). The February 11, 2020 post ( LA-RA reversal ). The March 18, 2020 post ( LA-RA reversal ).
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiac arrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). To EMPHASIZE: This pattern of diffuse Subendocardial Ischemia does not suggest acute coronary occlusion ( ie, it is not the pattern of an acute MI ).
There is no definite evidence of acute ischemia. (ie, Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. ( Some residual ischemia in the infarct border might still be present. Both episodes are initiated by an "R-on-T" phenomenon.
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia.
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy? How can you better assess the ST segments?
Contrary to what Ken stated, the ST vector remains mostly posterior __ What about subendocardial ischemia? Subendocardial ischemia results in ST depression, but unfortunately, and rather mysteriously, it does not localize to the ischemic wall. Similarly, STD in aVL is usually reciprocal to inferior ST elevation, not "lateral ischemia."
ACUTE MI (I allowed Acute MI to be in the report because I knew there would be an elevated troponin from ischemia, which is the definition of acute MI -- but in this case it would most likely be a Type 2 MI from tachycardia) There is also LA-RA lead reversal. The February 11, 2020 post ( LA-RA reversal ).
Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. In practice — It appears that electrical alternans is most often seen in association with regular SVT rhythms ( See the example in My Comment at the bottom of the page, in the September 7, 2020 post in Dr. Smith's ECG Blog ).
The primary endpoint of this study was major adverse cardiovascular and cerebrovascular events (MACCEs) that included all-cause mortality, non-fatal myocardial infarction, non-fatal ischemic stroke, and ischemia-driven revascularization.Results:The average age of the study participants was 59.55 ± 10.98 years, and men accounted for 61.8%.
Osborn waves have been reported with hypercalcemia, brain injury, subarachnoid hemorrhage, Brugada syndrome, cardiac arrest from VFib — and — severe, acute ischemia resulting in acute MI ( See My Comment in the November 22, 2019 post on Dr. Smith’s Blog ). Rituparna et al — as well as Chauhan and Brahma ( Int.
I thought this finding consistent with the finding of ST depression in lateral leads I; V4,V5,V6 — and possibly indicative of multivessel disease ( ie, Diffuse Subendocardial Ischemia — as discussed in ECG Blog #400 ). ECG Blog #400 — Reviews the concept of " dynamic " ST-T wave changes ( and also Diffuse Subendocardial Ischemia ).
The same reciprocal relationship is seen in severe subendocardial ischemia, just with opposite vector direction where V1 can show ST elevation) Below you can find the 3D model of the heart and coronary vessels. Each main coronary artery (LAD, RCA and LCx) are shown in separate images.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] There is evolution from Wellens Pattern A to Pattern B, now inclusive of V6.
Recognizing hyperacute T waves — patterns of leads — an OMI ( though not a STEMI ) — See My Comment at the bottom of the page in the November 8, 2020 post on Dr. Smith's ECG Blog. ECG Blog #400 — Reviews the concept of " dynamic " ST-T wave changes ( and also DSI = Diffuse Subendocardial Ischemia ).
It is due to transmural ischemia not only of the anterior wall and apex, but due to transmural ischemia of the septum, usually due to occlusion proximal to the first septal perforator. Is this Acute Ischemia? The voltage is high but not huge. Read the case. More on LVH. This is LVH only, not OMI. This is LVH Only, not OMI.
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. Ischemia can be disguised by a wide escape rhythm, which decreases the sensitivity of ECG.
--The STD in V2-V6 might be interpreted as subendocardial ischemia, but with the inferior STE, it is far more likely to represent posterior OMI. In subendocardial ischemia, cath lab is indicated if the pain persists in spite of medical therapy (aspirin, anticoagulant, IV nitro). At 100 minutes, the above ECG was recorded.
Learning Point: Concordant ST segment elevation can arise from profound ischemia triggered by ventricular tachycardia (VT), or it may represent an exaggerated basal ST change accompanying tachycardia. See My Comment at the bottom of the page in the May 19, 2020 post in Dr. Smith's Blog ). A peak troponin level of 70 ng/L was observed.
My interpretation was: RBBB with hyperacute T-waves in V4-V6 that are all but diagnostic of LAD occlusion vs. post ROSC ischemia. For more on the application of this Trace-down; Copy-over technique with Shark Fin ST segment deviations — See My Comment in the May 19, 2020 post in Dr. Smith's ECG Blog.
This ST depression appears to be maximal in leads V3-to-V5 — which could reflect acute posterior OMI ( O cclusion-based M yocardial I nfarction ) — most probably with multi -vessel disease ( ie, diffuse subendocardial ischemia suggested by the ST depression with ST elevation in aVR>V1 ). This patient has new CP — and — he is hypotensive.
5] Back to the case The patient had serial ECGs over the next hour with no significant change: The first troponin came back at 1,400 ng/L (normal <26 in males and <16 in females), confirming MI – and the patient’s refractory ischemia indicated this was an Occlusion MI.
There is a literature on this subject ( Sood et al — Cureus 15(4):e37102, 2023 — Gulati et al — Mayo Clin Proceed 95(1):136-156, 2020 — GGF van der Schoot et al: Neth Heart J 28(6):301-308, 2020 — and — Egred at al — Postgrad Med 81(962): 741-745, 2005 — to name just a few reports ). That said — acute MI does occur in younger patients.
There is probably a trickle of flow which is why there is both subendocardial ischemia (ST depression) and early subepicardial ischemia (hyperacute T-waves). Academic Emergency Medicine 27(S1): S220; May 2020. I sent the last one to the Queen of Hearts #PMCardio app and here is the verdict: My response: "It’s not even subtle.
Time 17 minutes Not much different One month earlier This is Left Bundle Branch Block (LBBB) without any sign of ischemia. If so, one would expect that the chest pain is diminishing or gone & that the culprit would be the LAD. It turns out that she spends much of her time in LBBB (see ECGs below) What is going on??? link] Shvilkin et al.
Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia. She was taken to the cath lab and her coronaries were clean!! There was no MRI, but the presumptive diagnosis is myocarditis. I have seen this pattern in severe acute AI also."
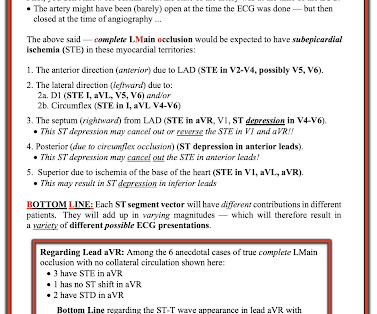
The terminology favored to describe these ECG findings is diffuse subendocardial ischemia ( See ECG Blog #271 — for more on diffuse subendocardial ischemia ). I discussed the findings of acute LMain occlusion further in My Comment in the January 16, 2020 post of Dr. Smith's ECG Blog. ECG Blog #316 — The patient died.
Here is the only prehospital 12-lead: Sinus tachycardia, somewhat wide QRS, Ischemia Here is the first ED ECG: What is the rhythm here? He was resuscitated into a perfusing rhythm. He went in and out of arrest until arrival at the ED.
I do not think this ECG is by itself diagnostic of OMI (full thickness, subepicardial ischemia ), b ut comparison to a previous might reveal this ECG as diagnostic of OMI. Thus, they obscure the last possible indication for emergent reperfusion in "NSTEMI" (all guidelines recommend emergent cath for refractory ischemia in NSTEMI).
ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ). ECG Blog #271 — Reviews determination of the ST segment baseline ( with discussion of the entity of diffuse Subendocardial Ischemia).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content