This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
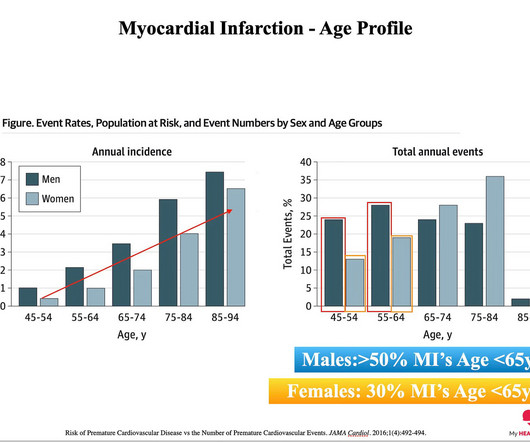
When you look at the risk of having a heartattack, it is true that the older you are, the greater the odds of having a heartattack 1. While only 1-2% of those having a heartattack are less than 65 years of age, 1-2% of this very large number means a LOT of heartattacks. So far, so good.
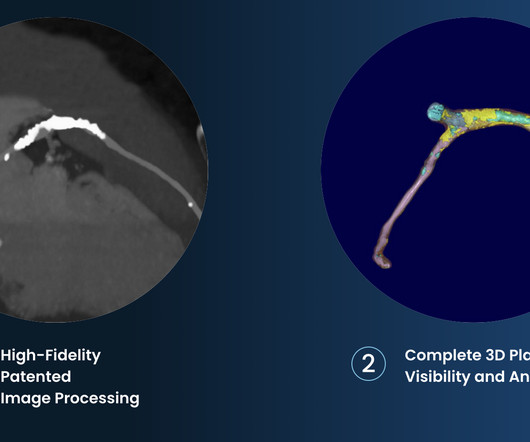
This registry will aim to provide world-wide physicians the most accurate information on coronary plaque to improve cardiovascular risk prediction and support the selection of patient-specific treatment,” said Dr. De Cecco. The ultimate goal is to positively impact cardiovascular health globally with a reduction in cardiovascular events."
Over a long enough time frame, pretty much everyone will get heart disease. By the time you get to age 80, you will almost certainly have evidence of plaque in your coronary arteries - you will have heart disease. But remember: Heart disease doesn’t kill people. Heartattacks do. Think decades.
To prevent heart disease, you need to know what causes it, how to measure the relevant factors and what to do about them. When we say heart disease, what we really mean is plaque in the artery wall. No heartattacks. That all depends on your overall risk of a future cardiovascular event like a heartattack.
Heart disease does not kill people. Heartattacks do. Appreciating this distinction is critical to understanding heart disease. Heart disease is the presence of plaque or atherosclerosis in the coronary arteries. In this instance, a heartattack. But does this approach work?
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heartattack or myocardial infarction (MI), stroke, and cardiovascular (CV) death.4
CT coronary angiography, in addition to a CT CAC, is arguably the best test for estimating whether someone has evidence of coronary artery disease and what that means for their near-term risk of a heartattack. Mixed Plaque - A combination of both calcified and NON-calcified plaque. More often than you would think!
Arteries generally narrow and occlude for one of two reasons: The progressive accumulation of plaque. A plaque ruptures, and a clot forms in the artery, thereby occluding it. The second reason is commonly referred to as a ‘HeartAttack’ or acute coronary syndrome. Prevent you from having a future heartattack.
Share Let’s first state our goal when we are in the business of ‘Heart Disease Prevention’: To delay the onset of coronary artery disease (atherosclerosis/plaque) that might rupture and cause a heartattack. And the less plaque you have, the lower the risk of a heartattack.
people from the general population), coronary artery calcium scores (CACS) are higher, indicating more calcification and the presence of atherosclerotic plaques. Calcified plaques are known to be more stable and less prone to rupture and lead to a heartattack. When comparing athletes to control groups (i.e.,
Subscribe now Stenting stable coronary artery disease has not been convincingly proven to reduce the risk of future heartattacks or death 1. The cause of angina usually involves inadequate blood flow reaching the heart muscle because of significant narrowing of the artery due to plaque buildup. All is fixed.
Only after her troponin peaked at 500,000 ng/L did she get her angiogram, which showed a 100% left main occlusion due to ruptured plaque. She died before she could get a heart transplant. They just could not believe that a young woman could have an OMI. RBBB, LAFB, and STE in I, aVL, V2 and V3. Diagnostic of Massive OMI.
He reports this was similar to how he felt when he had his heartattack 4 years prior, now s/p 4 stents. As per Dr. Smith this patient has known coronary disease from a previous MI, and in his words his CP ( C hest P ain ) felt "like his previous heartattack". We are not told how ECG #1 was interpreted.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content