This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
What do you think the echocardiogram shows? On echo, OMI has a wall motion abnormality, but SI usually does not. == MY Comment by K EN G RAUER, MD ( 5/13/2020 ): == It’s good to periodically review the differential diagnosis of the diffuse subendocardial ischemia. Cath lab activated Dual antiplatelet therapy and heparin given.
In comparison to the previous study, 11/11/2020, there has been a significant interval deterioration of left ventricular systolic function (previous EF 80%), and there is a new large apical wall motion abnormality. The estimated ejection fraction is 38%. Regional wall motion abnormality-apex, anterior akinesis.
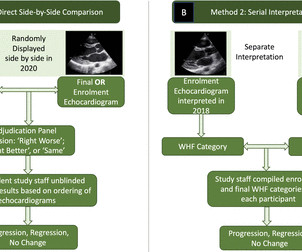
Methods A four-member expert panel reviewed 799 enrolment (in 2018) and completion (in 2020) echocardiograms from the GOAL Trial of latent RHD in Uganda to make consensus determination of normal, borderline RHD or definite RHD. Results There were 799 pairs of echocardiogram assessments included.
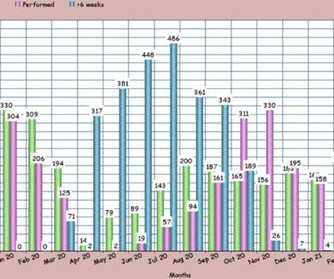
males), referred for a stress echocardiogram (SE), who underwent ESE between July 2020 (immediate post lockdown) and January 2021 according to national safety guidelines, in addition to patients wearing masks during ESE. at the start of July 2020 to the end of December 2020. SE service performance increased to 96.8%
Objective To identify the most common transthoracic echocardiogram (TTE) parameters in patients hospitalised with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2/COVID-19) and their association with myocardial injury and outcomes. Results A total of 87 patients met the eligibility criteria.
Before the procedure, patients should have an electrocardiogram (ECG) and echocardiogram (ultrasound of the heart) to check the heart’s rhythm and function. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS).
She underwent exercise echocardiogram in mid October where she exercised for nearly 7 minutes on the standard Bruce protocol and had typical anginal pain and shortness of breath. Baseline echocardiogram showed moderate LV systolic dysfunction with no wall motion abnormalities. There is inferoseptal hypokinesis.
Methods Patients were retrospectively evaluated between January 2012 and June 2020. Twenty-one (41%) had normal echocardiogram, 13 (25%) a hypokinetic non-dilated cardiomyopathy (HNDC) and 17 (33%) a dilated cardiomyopathy (DCM). Significant right ventricular involvement was an exclusion criterion.
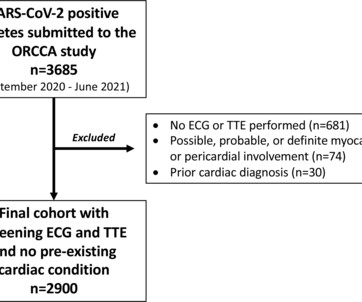
Methods The Outcomes Registry for Cardiac Conditions in Athletes was a nationwide prospective multicentre observational cohort study that captured testing and outcomes data from 45 institutions (September 2020–June 2021). Athletes with an ECG and transthoracic echocardiogram (TTE) and no pre-existing conditions were included.
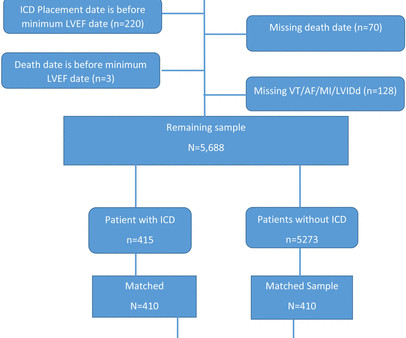
Methods Patients with lowest LVEF between 30% and 35% without an ICD prior to the lowest-LVEF echo (defined as ‘time zero’) were identified by querying echocardiography data from 28 November 2001 to 9 July 2020 at the Massachusetts General Hospital linked to ICD treatment status. vs 65.4%, p<0.0001), more often white (87.5%
A retrospective chart review was performed on 41 patients with COVID-19 on ECMO between March and October 2020. Twenty-two patients had transthoracic echocardiograms (TTE) completed while on ECMO (VV-ECMO = 19, VA-ECMO = 3). Echocardiograms (echo) were obtained pre-cannulation, during ECMO, and post-ECMO decannulation.
Additionally, a bedside echocardiogram showed no wall motion abnormality and normal LV function. A formal echocardiogram for patient 2 showed normal LV size, wall thickness, and global systolic function. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”.
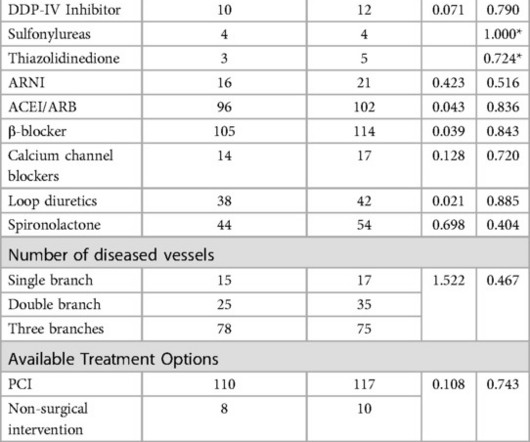
Two groups of patients' age, gender, diabetes duration, merge disease, echocardiogram and blood biochemical indexes, had no statistical difference (P>0.05). There were no significant differences in the number of coronary artery lesions, treatment regimens, cardiovascular and hypoglycemic drugs between the two groups (P>0.05).
Methods Patients from a large US hospital system undergoing combined LAAO and left-atrial CA from 8/2020 to 2/2024 were retrospectively analyzed and compared to a control group undergoing LAAO alone. vs. 4.5%, p =0.96) on transesophageal echocardiogram did not differ. vs. 2.1%, p =0.72) and minor (27.8%
The emergent echocardiogram showed normal EF, no WMA, and normal valve function. Alternatively — Today's regular SVT rhythm could be the much less common "fast-slow" form of AVNRT ( as I illustrate with laddergram in Figure-3 of My Comment in the March 6, 2020 post ). The angiogram showed completely normal coronary arteries.
from March 2020 to October 2021. Patients were included if they had: 1) acute COVID-19 infection confirmed by RT-PCR and 2) a transthoracic echocardiogram (TTE) performed during their hospitalization. Adult patients were identified by hospitalizations using ICD-10 code U07.1
Methods We retrospectively screened 2009 patients who underwent pacemaker implantation from 2010 to 2020 in seven institutions. The paced QRS recorded immediately after implantation was analyzed.
HCM is an "umbrella term" applied to the presence of LVH in the absence of "abnormal cardiac loading conditions" ( Hughes et al — JAHA 9:e015294, 2020 ). Cardiac cath showed normal coronary arteries.
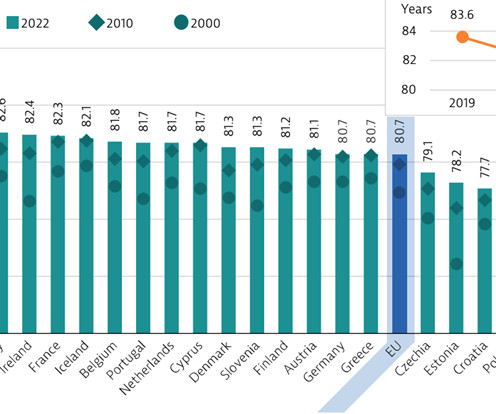
years, which has recovered well following a large decline due to COVID in 2020. For instance, the average waiting time for an echocardiogram at Turin’s Molinette Hospital was 31 days in 2016 and an even longer 53 days for a Holter ECG. In terms of healthcare spending, Italy allocates about 9.4%
Formal Echocardiogram: Normal left ventricular size and wall thickness. For more on the application of this Trace-down; Copy-over technique with Shark Fin ST segment deviations — See My Comment in the May 19, 2020 post in Dr. Smith's ECG Blog. Moderately decreased left ventricular systolic function with an estimated EF of 36%.
A rapid echocardiogram was performed, revealing an ejection fraction of 20% with thinning of the anterior-apical walls. See My Comment at the bottom of the page in the May 19, 2020 post in Dr. Smith's Blog ). The initial troponin T level was measured at 30 ng/L.
Elevated troponins prompted an echocardiogram — which revealed an apical wall motion abnormality (WMA). We have addresssed this issue on a number of occasions ( See My Comment in the April 25, 2023 — July 21, 2019 — December 10, 2019 — and January 10, 2020 posts). Patient #1 in today's post did not get expert ECG interpretation.
Formal echocardiogram: Systolic function is at the lower limits of normal. To add to this complexity ( as per My Comment in the August 22, 2020 post in Dr. Smith's ECG Blog ) — the ST-T wave appearance in repolarization variants may be dynamic ! This is a significant loss of myocardium and ejection fraction.
He had his echocardiogram done already and was normal. The 2020 “Padua Criteria” for Diagnosis and Phenotype Characterization of Arrhythmogenic Cardiomyopathy in Clinical Practice. I don’t know, whether a single blocked P could by any way a concealed Wenke -Bach. What does the guidelines say ? J Clin Med.
His echocardiogram showed normal wall motion. To paraphrase Dr. Smith's comments in the May 19, 2020 post : — Non-obstructive coronary disease does not ne cessarily imply no plaque rupture with thrombus. The patient did well afterward without any recurrence of symptoms. There are no further EKGs or troponin measurements.
Echocardiogram: The estimated left ventricular ejection fraction is 34% Regional wall motion abnormality-lateral, akinetic. She went to the cath lab and had a 100% Obtuse Marginal Occlusion (supplying the lateral and posterior wall) with TIMI-0 flow. A massive acute OMI.
Her contrast enhanced echocardiogram is shown below in the parasternal short axis view. Academic Emergency Medicine 27(S1): S220; May 2020. After returning from lab repeat troponin was 20,380 ng/L, and later that evening it peaked at 29,571 ng/L before trending down. The patient suffered a large infarct. Abstract 556.
He underwent formal echocardiogram several days later, which confirmed the findings of anterior, and apical wall motion abnormalities. Smith comment: this patient might have been sent home because of the poor sensitivity of this Point of Care (POC) assay. Do NOT use them. ng/mL when they stopped ordering further troponins. 1] Wereski, R.,
While awaiting transfer to the cath lab, STAT echocardiogram was performed and showed LVEF 30-35%, as well as anterior, inferior, and apical hypokinesis, and apical thrombus. The November 10, 2020 post — for PTA. The October 17, 2020 post — for a 70-year old woman with " Artifactual VT ". The thrombus is circled below in red.
Here is the post PCI EKG: And a few hours after that: The post PCI echocardiogram showed: Normal estimated left ventricular ejection fraction, 57%. This is a large OMI that has Zero ST Elevation but can be diagnosed by ECG features other than ST Elevation!! Regional wall motion abnormality-mid to basal inferior wall.
hours ECG: Not much change hs troponin I peaks at 500 ng/L 8 hours Next morning Urine drug screen: Amphetamine, Methamphetamine, Fentanyl, Fentanyl metabolite Formal Bubble Contrast Echocardiogram: Indications for Study: Silent Ischemia. SUMMARY Normal left ventricular cavity size. Normal estimated left ventricular ejection fraction.
She had an echocardiogram which was normal. Some General Thoughts on SVTs: I’ve previously reviewed in detail an approach to the regular SVT ( Please see My Comment — at the bottom of the page in the March 6, 2020 post in Dr. Smith’s ECG Blog ).
Echocardiogram: Estimated left ventricular ejection fraction, lower limits of normal; 45-50%. IF interested in more on the topic of fragmentation — See My Comment in the January 31, 2020 post. Tele Monitor: Normal sinus rhythm throughout, no ectopic atrial or ventricular beats. Regional wall motion abnormality-inferolateral.
The vaccine efficacy data for the original data was from thousands of patients and I certainly felt given the devastation wreaked on many of my patients in 2020 that the vaccines were the best chance of avoiding morbidity and mortality.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Smith on this blog ( Simply search for Brugada Syndrome! ).
This is a case written by Dan Lee (One of our fantastic Hennepin Residents, class of 2020 ) edits by Smith A 60 something-year-old man with a history of ESRD, LVH and prior CABG presented after an episode of hypotension during his hemodialysis, run followed by a syncopal episode which caused his run to be terminated early.
Echocardiogram: EF 50%, akinesis of mid-apical anteroseptal, inferior, and inferoseptal myocardium. Next morning: Slight evidence of reperfusion (or just completion) with terminal T wave inversion in many leads. QS waves from V2-V5 consistent with LV aneurysm morphology. Normal RV, no valve stenosis or regurgitation.
After discussing all of the above with ED staff, we have made a decision to get stat echocardiogram and assess overall LV function and wall motion abnormalities and defer cath lab activation at the time." On the other hand, stable EKG over an hour in the setting of ongoing acute coronary syndrome is again unusual.
Next day, a stress echo was done: The exercise stress echocardiogram is normal. Normal estimated left ventricular ejection fraction improved with stress. No wall motion abnormality at rest. No wall motion abnormality with stress. The stress electrocardiogram is non-diagnostic. The patient did not report angina with stress.
I have ordered an echocardiogram which will be done today, after that patient can be discharged to home with follow-up in 2 to 3 months." The echo was normal. Learning points 1. In this regular wide complex tachycardia , since the rhythm converted w adenosine, it is almost certainly SVT w aberrancy, which can be either: A.
Here is the cath report: Echocardiogram: There is severe hypokinesis of entire LV apex and apical segment of all the walls. For review of ECG findings expected with Takotsubo Cardiomyopathy — Please see My Comment at the bottom of the page in the March 25, 2020 post in Dr. Smith's ECG Blog ). ng/mL by 4th generation and older assays.)
It is relevant to note here that as a physician active clinically in both the inpatient and outpatient arenas, I am an eyewitness to the severe toll COVID19 took on my patients in the Spring or 2020. He has had COVID twice, first in September of 2020, and his second time in January of 2023. The pain resolved a few weeks later.
Later, he underwent a formal echocardiogram: Very severe left ventricular enlargement (LVED diameter 7.4 Figure-4: I’ve postulated a laddergram for ECG #3 in Today’s Case ( For more on the use of laddergrams — See My Comment in the February 20, 2020 post ). The patient was given furosemide and admitted to the hospital.
She needs an echocardiogram to rule out any subclinical myocardial disease. Echocardiogram is a must. 2020 Aug;43(8):827-833. 2020 Aug;43(8):827-833. Epub 2020 Apr 7. (Rarely, neuro-adrenergic-emotional signals from brainstem can tilt the ST segment like this. Have seen a HCM variants like this ).TMT Reference 1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content