This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Short-long-short (S-L-S) electrocardiographic cycle length patterns are associated with incidence of ventricular tachycardia (VT) and ventricular fibrillation (VF). It is also recognised that pacemakers can facilitate these cycle length sequences, and that the observation of these sequences can predict future VT/VF events.
She was successfully revived after several rounds of ACLS including defibrillation and amiodarone. An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). In particular — QRS alternans during narrow SVT rhythms has been associated with reentry tachycardias.
The rhythm is regular — at a rate just over 100/minute = sinus tachycardia ( ie, the R-R interval is just under 3 large boxes in duration ). Continuing with assessment of ECG #1 in Figure-2: The rhythm is sinus tachycardia at ~110/minute. A series of VFib episodes followed — each time with successful defibrillation.
After resuscitation and defibrillation , there were no more episodes of TdP. Below is the patient’s 12 lead ECG following defibrillation. But there are 3 other wide beats in the tachycardia that begins with beat #6 ( = beats #7; 13,14 ). NT-proBNP was significantly elevated at 4900ng/L ( ref < 500ng/L ).
She was never defibrillated. 3 of the 4 have similarly bizarre PVCs. == MY Comment by K EN G RAUER, MD ( 4/29/2020 ): == Cardiac Arrest with Bizarre PVCs/Torsades de Pointes: Intriguing case with many interesting features. As was seen in this case — defibrillation and/or overdrive pacing may be needed. What do you think?
He was found in ventricular fibrillation and defibrillated, then brought to a local ED which does not have a cath lab. I’ve previously discussed clinical application of the Mirror Test on several occasions ( SEE My Comment at the bottom of the page in both the September 13, 2020 post and the February 16, 2019 post in Dr. Smith’s ECG Blog ).
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. She was given CRT-D (Cardiac Resynchronization Therapy-Defibrillator). During the next 24 hours, she experienced periods of complete AV block with a ventricular escape rhythm in the 20s. She was started on isoprenalin (isoproterenol).
IMPRESSION: Given the presence of a wide tachycardia — with 2 distinct QRS morphologies, and no sign of P waves — a presumed diagnosis of B i D irectional Ventricular Tachycardia has to be made. Despite prolonged resuscitation with multiple defibrillation attempts — the patient could not be saved. =
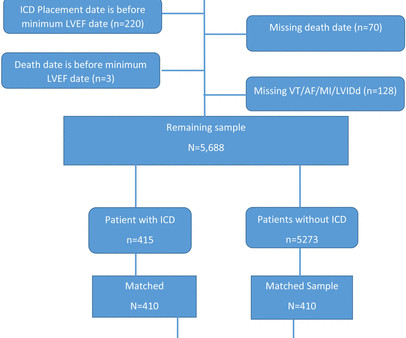
Background Consensus guidelines support the use of implanted cardioverter-defibrillators (ICD) for primary prevention of sudden cardiac death in patients with either non-ischaemic or ischaemic cardiomyopathy with left ventricular ejection fraction (LVEF) ≤35%. vs 65.4%, p<0.0001), more often white (87.5% vs 38.2%, p<0.0001).
There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). This episode self terminated before defibrillation was possible. This run of TdP is initiated by a PVC — but it then self-terminates. Discussion : The patient in today’s case presented with "seizures".
The arrhythmia spontaneously converted before defibrillation was achieved. Figure-1: Reasons for the varied ECG presentation of acute LMain occlusion — excerpted from Dr. Smith’s 8/9/2019 post ( This Table from My Comment in the January 16, 2020 post ). ECG #3 The above ECG shows a polymorphic VT at a rate of about 180 BPM.
The team immediately paged cardiology, concerned for polymorphic ventricular tachycardia. Since sinus conducted QRS complexes cannot co-exist together with ventricular tachycardia, this must all be artifact. The November 10, 2020 post — for PTA. The October 17, 2020 post — for a 70-year old woman with " Artifactual VT ".
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). He required multiple defibrillations within a period of a few hours. An ICD ( Implantable Cardioverter Defibrilator ) was placed prior to discharge. What do you think?
We can see enough to make out that the rhythm is sinus tachycardia. Tachycardia is unusual for OMI, unless the patient is in cardiogenic shock (or getting close). A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. She was ventilated by bag-valve-mask by EMS on arrival and was quickly intubated with etomidate and succinylcholine. A rectal temperature was obtained which read 107.9
Smith comments : Wide complex tachycardia. The differential diagnosis of WCT is: 1) Sinus tachycardia with "aberrancy" (in this case RBBB and LAFB), but there are no P-waves and the QRS morphology is not typical of simple RBBB/LAFB. Also, if the rate is constant, not wavering up and down, it is highly unlikely to be sinus tachycardia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content