This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
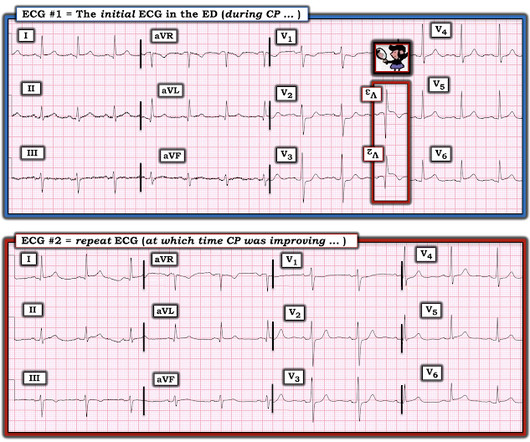
Written by Jesse McLaren A healthy 75 year old developed 7/10 chestpain associated with diaphoresis and nausea, which began on exertion but persisted. Below is the first ECG recorded by paramedics after 2 hours of chestpain, interpreted by the machine as “possible inferior ischemia”. What do you think?
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). As a result, this 45-year old man did not experince any delay in treatment — and a large diagonal branch of the LAD was stented with good outcome.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? What do you think? This was the cost of preventing infarction of the anterior wall.)
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset.
A 50-something man presented in shock with severe chestpain. Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. The February 11, 2020 post ( LA-RA reversal ). The March 18, 2020 post ( LA-RA reversal ). The August 28, 2020 post ( LA-LL reversal ).
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. A single DES stent was placed, and the patient did well post-procedure.
The logic of stenting obstructed coronary arteries is simple. A stent unblocks the artery. Subscribe now Stenting stable coronary artery disease has not been convincingly proven to reduce the risk of future heart attacks or death 1. But coronary stenting is not the only way to reduce symptoms of angina. All is fixed.
A 50-something with no previous cardiac history and no risk factors presented to the ED with acute chestpain (pressure) that radiated to the left arm. It was stented with good results. An ECG was immediately recorded: Computer read: Normal ECG What do you think? There is ST depression in V1-V3.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, Pericarditis would be even more unlikely in someone without chestpain.
== MY Comment by K EN G RAUER, MD ( 9/17/2020 ): == Todays patient is a previously healthy, 60-something year-old woman who presented with chestpain that began at a reception. We are indebted to Dr. Smith for developing Modified Smith-Sgarbossa Criteria for assessing ST-T wave changes in chestpain patients with LBBB.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
One of the most common questions I get is, “ Do I need a stent to treat my heart disease?” ” Typically, several of this person’s friends have had stents, so it seems natural to ask. First, we must understand what a stent is and why it is used. The stent ‘unblocks’ it. Flow is restored.
As discussed in many posts in this ECG Blog — despite not satisfying the millimeter-based definition of a STEMI — in this patient with new chestpain, the ECG findings in Figure-1 merit prompt cath lab activation without any need to wait for serum troponin to return elevated ( See ECG Blog #193 — regarding the new "OMI" paradigm ).
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chestpain described as an “explosion" of left chest pressure. Today’s pain lasted around 20 mins, but was severe enough that the patient called EMS. Triage EKG: What do you think? 1] Wereski, R.,
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. Echo showed new anterior regional wall motion abnormality and decrease EF from 60% to 45%.
Sent by anonymous A man in his 40s with no previous heart disease presented within 30 minutes of onset of acute chestpain that started while exercising. Successful drug-eluting stent placement opening up 95% mid RCA stenosis to 0% residual Nonobstructive left system disease. Chestpain and a computer ‘normal’ ECG.
The patient's chestpain had resolved by the time of the ECG 2. But it does prove that the patient has coronary disease and makes the probability that his chestpain is due to ACS very very high. Angiogram: Widely patent RCA and LAD stents. Therefore, no stent was placed. (No There are well-formed Q-waves 3.
There is new data showing better outcomes when bystander lesions (non-culprit) are stented. == MY Comment by K EN G RAUER, MD ( 8/28/2020 ): == Dr. Smith highlights a number of important lessons to be learned from today’s case. August 30, 2020 ): Being an “expert” in ECG interpretation is sometimes very humbling.
See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. This is different from nitroglycerin which produces vasodilation and can improve by pain improving myocardial perfusion. Here is the angiogram after stent placement. See this case: A man his 50s with chestpain. At midnight.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. It was stented. This was a large OMI.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chestpain that started within the last hour. The patient was found to have total "mid" LAD occlusion which was stented: Pre-PCI. Both were awake and alert with normal vital signs. What do you think? The cath lab was now activated.
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chestpain. EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chestpain from an 8/10 to 4/10. The ECG only tells you there is ischemia, not the etiology of it.
Decision was made to stent the lesion. There was never any severe chestpain. We review ECG findings in Takotsubo Cardiomyopathy in the March 25, 2020 post of Dr. Smith's ECG Blog. The following day in the cath lab a borderline significant mid LAD stenosis was found. Are these reperfusion T waves from transient OMI ?
Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery. Regardless, if you present with chestpain and get a stress test instead of a CTCA, you are arguably getting an inferior test. I would say yes.
This middle aged male with h/o GERD but also h/o stents presented to the ED with chestpain. The initial troponin I returned at 1500 ng/L and another ECG was recorded as the patient complained of 9/10 chestpain at 10 hours after the first Now the T-wave in III is fully upright, suggesting re-occlusion.
Case 1 A middle aged woman presented with acute chestpain and shortness of breath, unclear time since onset, and likely with episodic symptoms off and on throughout the day. Another lesion in the proximal LAD with 80% stenosis was stented as well. Culprit lesion was reduced to 0% and stented. Additional case by Smith.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
This is a case written by Dan Lee (One of our fantastic Hennepin Residents, class of 2020 ) edits by Smith A 60 something-year-old man with a history of ESRD, LVH and prior CABG presented after an episode of hypotension during his hemodialysis, run followed by a syncopal episode which caused his run to be terminated early. No chestpain.
It was opened and stented. The reason the initial ECG is so concerning — is that it already suggests high likelihood of OMI ( = O cclusion-based MI ) in this 50-ish year old man who presents with a 2-hour history of new chestpain. Formal bubble contrast echo: The estimated left ventricular ejection fraction 57%.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
The patient contacted EMS after a few hours of chestpain that started 5:30 AM. The pain was described as 6/10 radiating to the right shoulder. The chestpain was described as both sharp and pressure like. The culprit lesion was opened and stented. He is otherwise healthy.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. She presented to the emergency department after a couple of days of chest discomfort. She also has a hx of paroxysmal atrial fibrillation and is on oral anticoagulant treatment. The last echocardiography 12 months ago showed HFmrEF.
It was stented. 12 Example Cases of Use of 3- and 4-variable formulas, plus Simplified Formula, to differentiate normal STE from subtle LAD occlusion 3. . == == MY Comment by K EN G RAUER, MD ( 10/23/2020 ): == There are a number of important lessons worthy of repeating from today's repost of our case from March 28, 2017.
Delayed angiogram found a 95% mid RCA occlusion that was stented. Smith's ECG Blog — I've found use of the Mirror Test to be extremely helpful in facilitating visualization of the ST-T wave changes characteristic of acute Posterior MI ( See My Comment at the bottom of the page in the September 21, 2020 post).
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. The patient has acute persistent refrectory chestpain and elevated troponin.
He contacted EMS due to acute onset chestpain and feeling unwell and fatigued. He subsequently developed worsening chestpain. This, in the context of worsening chestpain , is evidence of reocclusion of the infarct-related artery and active OMI in development. The below ECG was recorded. What do you think?
Case A 76 year old man with chronic hypertension but no history of coronary disease or myocardial infarction presented to the ED with chestpain at 2343. It was treated with a drug eluting stent. It is awaiting FDA approval (but approved for 1.5 There is ST elevation in the inferior leads.
Written by Pendell Meyers An adult man presented with acute chestpain. He had undergone stenting of the LAD several weeks ago (unclear whether elective for stable symptoms, or in response to acute coronary syndrome). Acute chestpain, right bundle branch block, no STEMI criteria, and negative initial troponin.
A 50 something male presented in the evening to ED for evaluation of chestpain that started at 1600. He reports this was similar to how he felt when he had his heart attack 4 years prior, now s/p 4 stents. The chestpain continued for hours. The patient was still having chestpain.
The patient contacted the ambulance service after he experienced sudden onset chestpain and diaphoresis that had started 20 minutes prior. At cath there was a 100% proximal LAD occlusion, which was opened and stented. The above ECG is from man in his 80s with crushing chestpain. Troponin T peaked at 9378 ng/L.
A 62 year old man with hyperlipidemia presented to a rural emergency department with 7 hours of 3/10 chestpain. The proximal and mid LAD stenoses were stented and the OM 2 was left alone. In fact, much of what passes for EKG education can actually harm one's interpretation skills.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chestpain. After stent placement: The vessel is now open with TIMI 3 flow, although it is diffusely diseased and the middle segment is ectatic.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content