This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
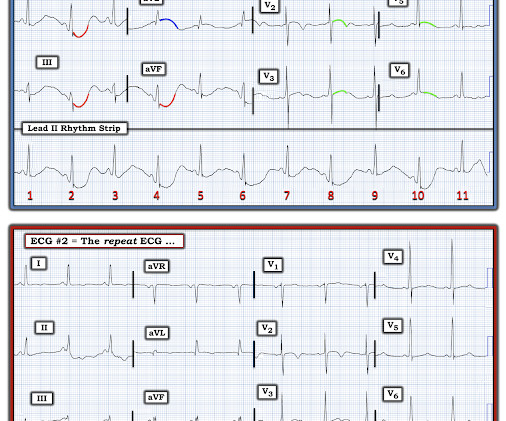
A 60 year old with chestpain presented to the ED. In this case, lead I does not look bizarre, but all other leads do. == N OTE : The reasons I especially liked today's case are: i ) The patient presented with chestpain — so the importance of distinguishing artifact from reality can not be overstated! —
Impression: In this middle-aged man with palpitations and dyspnea, but no chestpain — I suspect that the T wave peaking and slight, upward-sloping chest lead ST elevation represent a repolarization variant. The February 11, 2020 post ( LA-RA reversal ). The March 18, 2020 post ( LA-RA reversal ).
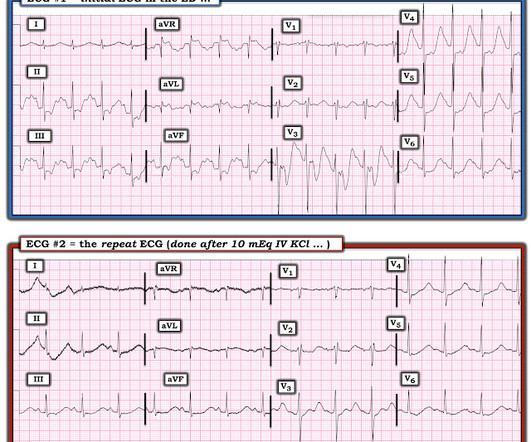
Figure-1: The initial ECG in today's case — obtained from a 50-year old man with new chestpain. ( In contrast — it is EASY to overlook L A- L L reversal — because the ECG picture seen with this type of lead reversal does not immediately stand out as physiologically “off”. The February 11, 2020 post ( LA-RA reversal ).
AV synchrony and physiologic ventricular depolarization the hemodynamics improved. Lowering the back up rate (LRL) of the ICD/pacer allowed for an intrinsic rhythm with physiologic AV conduction and normal AV synchrony with resultant increase in stroke volume and cardiac outpt.
The patient had come to the ED for SOB, but without any chestpain. Global hypokinesis with possible regional wall motion abnormality-inferior & inferolateral Compared to the Echo from 10/2020, there has been a significant interval change: 1. Therefore, as many as 11 of the 12 leads can look bizarre.
And some similar ECGs from Pulmonary Embolism: A young woman with altered mental status and hypotension An elderly woman transferred to you for chestpain, shortness of breath, and positive troponin - does she need the cath lab now? It just doesn’t make physiologic sense to have deep T wave inversion in V1 and V3, but not in V2.
There was no chestpain. I’ve reviewed My Take on the ECG diagnosis of RVH on a number of occasions in Dr. Smith’s ECG Blog ( See My Comment at the bottom of the page in the March 6, 2022 and September 1, 2020 posts , to name just 2 ). But today's patient had no chestpain. How Does this Apply to Today’s Case?
Written by Pendell Meyers, with edits by Smith A man in his 80s presented with acute chestpain and normal vital signs. We need more such ECGs for training but we are constantly working on the algorithm and one day it will make this diagnosis. == But isn't ongoing chestpain in NSTEMI a guideline indication for emergent angiography?
There was no chestpain. The physiologic reason for this — is thought to be the result of momentarily increased circulation from mechanical contraction arising from the "sandwiched in" QRS complex. This was written by Magnus Nossen The patient is a female in her 50s. She presented with a one week hx of «dizziness» and weakness.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content