This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
For example, considering whatever symptoms that the patient may have had ( ie, chestpain, palpitations, shortness of breath, etc. ) — what this might mean in view of the ECG we are looking at. STEP #2 = Clinical Impression — in which we correlate our assessment that we made in Step #1 to the clinical situation at hand.
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chestpain. The patient is a young adult male with chestpain. The chestpain was described as pressure like and radiation to both arms and the jaw. How would you assess this ECG? What is your next step?
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chestpain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands.
Written by Jesse McLaren A healthy 75 year old developed 7/10 chestpain associated with diaphoresis and nausea, which began on exertion but persisted. Below is the first ECG recorded by paramedics after 2 hours of chestpain, interpreted by the machine as “possible inferior ischemia”. What do you think?
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). We have addresssed this issue on a number of occasions ( See My Comment in the April 25, 2023 — July 21, 2019 — December 10, 2019 — and January 10, 2020 posts).
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? What do you think?
Written by Jesse McLaren A 50 year old presented to triage with one hour of chestpain, and the following ECG labeled normal by the computer (GE Marquette SL) algorithm. What do you think? Theres normal sinus rhythm, first degree AV block, early R wave, normal voltages. Here is her ECG: What do you think?
I went to the patient's chart: Elderly woman with stuttering chestpain and SOB, and dizziness. For more on Giant T waves — See My Comment at the bottom of the page in the June 22, 2020 and September 19, 2022 posts in Dr. Smith's ECG Blog ). What do you think now? This is a very typical ECG for Hypertrophic Cardiomyopathy.
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Do either, both, or neither have occlusion MI? Vitals were normal.
A 60-something yo female presented w/ exertional chestpain for 3 days. Pain was 8/10 and constant. She has been experiencing progressively worsening exertional dyspnea and chest tightness mostly when climbing up flights of stairs since early September. But the patient has active chestpain.
Let me tell you about her hospitalization, discharged 1 day prior, but it was at another hospital (I wish I had the ECG from that hospitalization): The patient is 40 years old and presented to another hospital with chestpain and SOB. She had been sitting doing work when she experienced "waves of chest tightness". Sats were 88%.
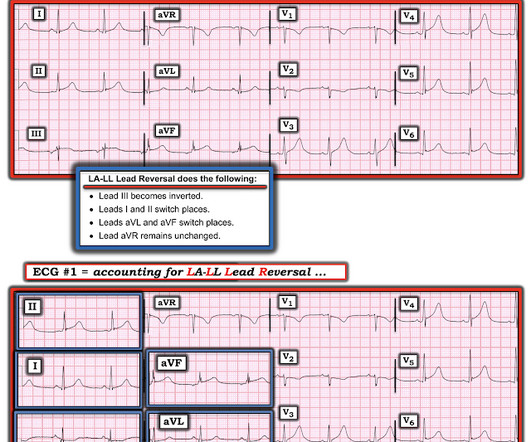
A 50-something man presented in shock with severe chestpain. The February 11, 2020 post ( LA-RA reversal ). The March 18, 2020 post ( LA-RA reversal ). The August 28, 2020 post ( LA-LL reversal ). The November 19, 2020 post ( LA-LL reversal ). His prehospital ECG was diagnostic of inferior posterior OMI.
There were no injuries and no chestpain and he appeared well. He complained of 3 days of diarrhea and abdominal pain. Pretest probability: Especially when there is no Chestpain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear.
Case sent by Logan Stark MD, written by Pendell Meyers A woman in her 70s presented with acute chestpain. As I emphasize in my September 26, 2020 post of Dr. Smith's ECG Blog — the most common cause of a pause is a blocked PAC ( and not some form of AV block ). No prior ECG was available. This left 2 additional considerations.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Altogether, this strongly suggests inferolateral OMI, particularly in a patient with acute chestpain.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Triage VS: 135/65 mmHg, 95 bpm, 94% on room air, 16/min, 98.6 Abstract 556.
Sent by Drew Williams, written by Pendell Meyers A man in his 50s with history of hypertension was standing at the bus stop when he developed sudden onset severe pressure-like chestpain radiating to his neck and right arm, associated with dyspnea, diaphoresis, and presyncope. EMS arrived and administered aspirin and nitroglycerin.
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. PEARL: Most patients who present with new chestpain + ECG changes + positive troponin — will not need Cardiac MRI. This was sent to me by a partner: "Curious what you think of this one we had overnight.
My Comment by K EN G RAUER, MD ( 2/22 /2023 ): = Today’s case is an important one, because as per Dr. Smith ( in this patient with new chestpain ) — “The initial ECG is diagnostic of infero-postero OMI.” The presence or absence of ST Elevation is a poor marker with which to describe a myocardial infarction. =
Background Despite the crucial role of Chestpain centers (CPCs) in acute myocardial infarction (AMI) management, China's mortality rate for ST-segment elevation myocardial infarction (STEMI) has remained stagnant. The cohort was stratified by Killip classification at admission (Class 1: n = 402, Class ≥2: n = 262).
A 60 year old with chestpain presented to the ED. In this case, lead I does not look bizarre, but all other leads do. == N OTE : The reasons I especially liked today's case are: i ) The patient presented with chestpain — so the importance of distinguishing artifact from reality can not be overstated! —
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
The patient presented with chestpain. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. Only 5-18% of ED patients with chestpain have a myocardial infarction of any kind. Is it Brugada pattern?
A 50-something with no previous cardiac history and no risk factors presented to the ED with acute chestpain (pressure) that radiated to the left arm. But even without these additional findings — the "Must Recognize" ECG pattern in this patient with new chestpain — is the unmistakeable shape of the ST depression in leads V2 and V3!
There is a patient with persistent chestpain and an initial troponin I over 52 ng/L; 52 ng/L has an approximate 70% PPV for acute type I MI in a chestpain patient. Pain was severe and persistent. CT angiography chest assessing for PE and dissection negative. Heparin drip was initiated. Is there STEMI?
Written by Jesse McLaren Two 70 year olds had acute chestpain with nausea and shortness of breath, and called paramedics. Int J Cardiol Heart Vasc 2020 3. Today's patient is a 70-year old adult who called EMS because of new-onset chestpain , associated with nausea and shortness of breath. Who needs the cath lab?
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. He has a medical hx notable for hypertension, hyperlipidemia and previous tobacco use disorder.
Upon questioning patient, he denies having any chestpain or chest tightness of any sort. In the absence of chestpain and negative troponin , it appears less likely that he is having acute coronary syndrome though EKG appears concerning. Pericarditis would be even more unlikely in someone without chestpain.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Am J Emerg Med 2020 3. Int J Cardiol 2013 2.
== MY Comment by K EN G RAUER, MD ( 9/17/2020 ): == Todays patient is a previously healthy, 60-something year-old woman who presented with chestpain that began at a reception. We are indebted to Dr. Smith for developing Modified Smith-Sgarbossa Criteria for assessing ST-T wave changes in chestpain patients with LBBB.
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chestpain and shortness of breath after finishing a 4-mile run. His symptoms of chestpain and shortness of breath were attributed to an asthma exacerbation during exercise.
A 30-something male presented in the middle of the night with several hours of sharp, non-radiating, left sided chestpain. But this is not the mix-up that occurred in today’s case — because we do not see global negativity ( of P wave, QRS and T wave ) in lead I ( See the February 11, 2020 post). I initially missed that one.
Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS.
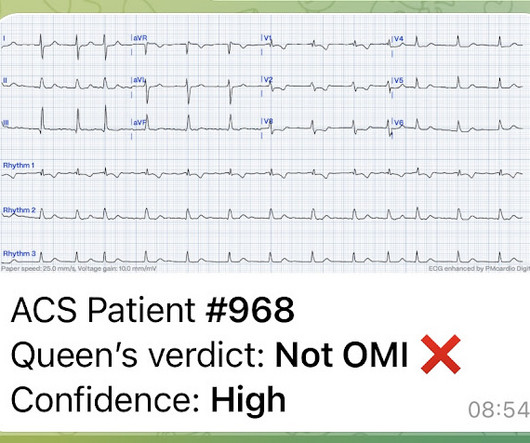
An 80-something woman who presented with chestpain and dyspnea. That said — QOH is already highly sophisticated and accurate in her assessment of ECGs from acute chestpain patients, in which the ECG is not complicated by uncommon OMI mimics. After all, this patient did also present with chestpain. ) — See below.
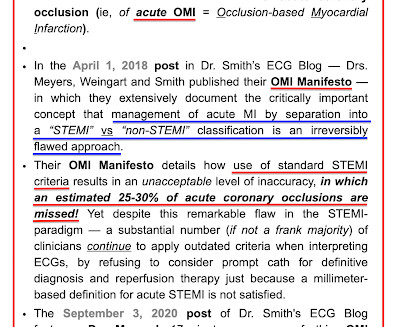
It is from a 50-something with chestpain: What do you think? Up until recently — all computerized ECG interpretation programs that I am aware of used standard millimeter-based STEMI critieria as the basis for determining which chestpain patients should "qualify" for prompt cath with PCI. This was sent to me by a friend.
Impression: In this middle-aged man with palpitations and dyspnea, but no chestpain — I suspect that the T wave peaking and slight, upward-sloping chest lead ST elevation represent a repolarization variant. The February 11, 2020 post ( LA-RA reversal ). The March 18, 2020 post ( LA-RA reversal ).
Written by Pendell Meyers, with some edits by Smith A man in his 40s with many comorbidities presented to the ED with chestpain, hypotension, dyspnea, and hypoxemia. An 80-something woman who presented with chestpain and dyspnea. Here is his triage ECG: What do you think? Lots of info here.
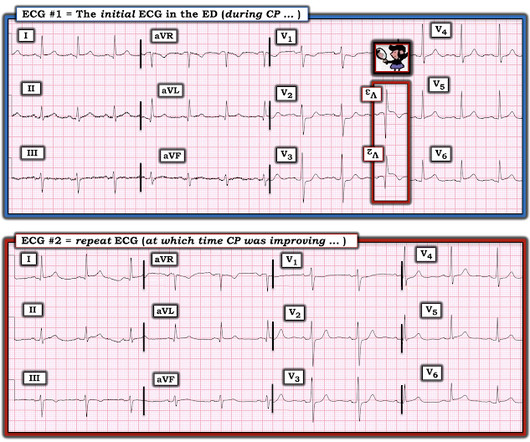
== MY Comment by K EN G RAUER, MD ( 8/22/2020 ): == The patient is a mid-50s man who presented to the ED for new-onset chestpain of ~1 hour duration. He was still having chestpain in the ED at the time ECG #1 was done ( Figure-1 ). His symptoms awakened him from sleep. The cath lab was not activated at this time.
For full discussion of this case — See ECG Blog #292 — == The 2 ECGs shown in Figure-1 were obtained from a man in his 30s — who presented to the ED ( E mergency D epartment ) with chestpain that began several hours earlier. ECG #2 was recorded 1 hour after ECG #1. Initial troponin was negative.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chestpain described as an “explosion" of left chest pressure. Today’s pain lasted around 20 mins, but was severe enough that the patient called EMS. Triage EKG: What do you think? 1] Wereski, R.,
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
As discussed in many posts in this ECG Blog — despite not satisfying the millimeter-based definition of a STEMI — in this patient with new chestpain, the ECG findings in Figure-1 merit prompt cath lab activation without any need to wait for serum troponin to return elevated ( See ECG Blog #193 — regarding the new "OMI" paradigm ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content