This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
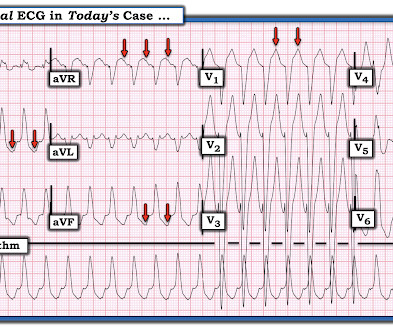
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation.
Working through a case of a regular WCT Rhythm in this 80-something woman See My Comment in the May 5, 2020 post on Dr. Smiths ECG Blog. Another case of a regular WCT Rhythm in a 60-something woman See My Comment at the bottom of the page in the April 15, 2020 post on Dr. Smiths ECG Blog. Smiths ECG Blog.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. Analysis: there is a wide complex tachycardia. This was the interpretation I put into the system: WIDE COMPLEX TACHYCARDIA. It is regular.
His previous echo one month prior shows the same thing: “consistent with old infarct in LAD vascular territory, with EF 45%” "I think there is something else causing his tachycardia which is exaggerating his EKG findings and mimicking an acute myocardial infarction." He had a h/o ischemic cardiomyopathy and right MCA stroke.
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
Conventional algorithm interpretation: SINUS TACHYCARDIA ABNORMAL RHYTHM ECG Confirmed by over-reading physician Transformed ECG by PM Cardio: PM Cardio interpretation: OMI with Low Confidence Dr. Rob Reardon did a bedside echo using Speckle tracking. (see Stress induced cardiomyopathy (Takotsubo like LV dysfunction) possible.
But for those wanting a "simpler" approach" — Consider the following ( which I review below in my ADDENDUM ): This patient is in a wide, "ugly-looking" and seemingly regular tachycardia without P waves. Working through a case of a regular WCT Rhythm in this 80-something woman — See My Comment in the May 5, 2020 post on Dr. Smith’s ECG Blog.
Here was the ECG: There is sinus tachycardia. In other words, the severely increased end diastolic pressure from the extremely poor LV function caused by the myocarditis results in extremely poor coronary perfusion pressure. == MY Comment by K EN G RAUER, MD ( 2/16/2020 ): == As per the title by Dr. Smith — this case was not what I thought.
The patient was diagnosed with stress cardiomyopathy. Widespread T wave inversions and prolongation of the QT interval is not uncommon in Takotsubo cardiomyopathy. The QTc then gradually shortened over the course of several days as is usual for stress cardiomyopathy. Potassium was 4,8 mmol/l. ( ref 3,5-4,6 mmol/l ).
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( Takotsubo (ie, Stress ) Cardiomyopathy. How would YOU interpret this tracing?
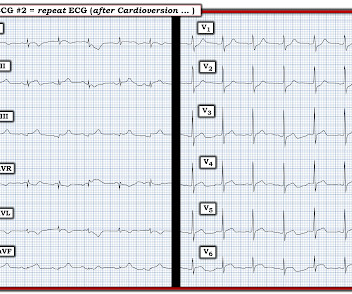
Given the rapid rate of the tachycardia and the amorphous shape of the QRS — the decision was made to sedate the patient and cardiovert. This phenomenon may sometimes be seen following an episode of a sustained tachycardia — in which marked ST-T wave abnormalities not due to infarction may be seen for a period of hours, or even days!
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
Hypertrophic Cardiomyopathy or Normal ("Variant")? T-wave inversions and dynamic ST elevation Tachycardia, hyperthyroid, and ST elevation. Potential Adverse Cardiovascular Effects From Excessive Endurance Exercise Exercise Is Medicine? The Cardiorespiratory Implications of Ultra-marathon Bjørkavoll‐Bergseth et al. What is it?
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. The granulomatous inflammation affects the heart, causing an infiltrative cardiomyopathy The most common manifestations of cardiac sarcoidosis are atrioventricular (AV) block and ventricular tachyarrhythmias (VT).
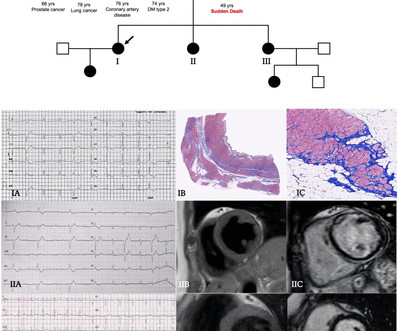
Objectives To describe a cohort of patients with arrhythmogenic left ventricular cardiomyopathy (ALVC), focusing on the spectrum of the clinical presentations. Methods Patients were retrospectively evaluated between January 2012 and June 2020. Results Fifty-two patients (63% males, age 45 years (31–53)) composed the study cohort.
Arrhythmogenic cardiomyopathy Long QT syndrome Hypertrophic cardiomyopathy. There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). There are a number of things to look for in an ECG that can hint at arrhythmia as the cause of an apparent seizure.
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. The absence of any wall motion abnormality makes ischemic cardiomyopathy very unlikely. An ECG was recorded: This shows a regular narrow complex tachycardia at a rate of about 160. BP:143/99, Pulse 109, Temp 37.2 °C
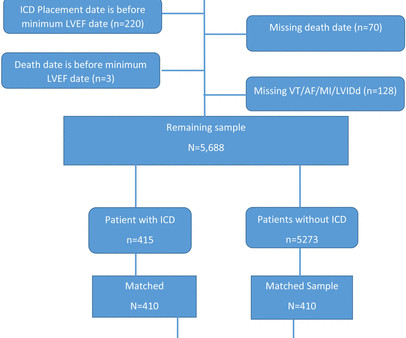
Background Consensus guidelines support the use of implanted cardioverter-defibrillators (ICD) for primary prevention of sudden cardiac death in patients with either non-ischaemic or ischaemic cardiomyopathy with left ventricular ejection fraction (LVEF) ≤35%. vs 65.4%, p<0.0001), more often white (87.5% vs 38.2%, p<0.0001).
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. JAMA Cardiol [Internet] 2020;Available from: [link] 4. JAMA Cardiol [Internet] 2020;Available from: [link] 5. Guo T, Fan Y, Chen M, et al.
See this even more interesting and more dramatic and fascinating case: History of Hypertrophic Cardiomyopathy (HOCM), with Tachycardia and High Lactate = My Comment by K EN G RAUER, MD ( 10/28 /2023 ): = QUESTION: For clarity in Figure-1 — I've reproduced today's ECG without the long lead rhythm strip. 23/WCC — 2/21/2020 ).
However, the effects of sacubitril/valsartan on these outcomes, as well as on ventricular tachyarrhythmias, have not been well studied in women with HFrEF.MethodsThis study included consecutive series of patients treated with sacubitril/valsartan at University Hospital Mannheim from 2016 to 2020. were ambulatory and 51.4% were hospitalized.
Other than tachycardia, Other than slight tachycardia, vitals were within normal limits (including oxygen saturation). As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. Is that normal?
Smith comments : Wide complex tachycardia. The differential diagnosis of WCT is: 1) Sinus tachycardia with "aberrancy" (in this case RBBB and LAFB), but there are no P-waves and the QRS morphology is not typical of simple RBBB/LAFB. Also, if the rate is constant, not wavering up and down, it is highly unlikely to be sinus tachycardia.
The relationship between J wave and ventricular tachycardia during Takotsubo cardiomyopathy. Internat J Arrhyth 2020 Uesako H, Fukikawa H, Hashimoto S, et al. When due to ischemia — Osborn waves may be associated with high risk of developing malignant ventricular arrhythmias ( My Comment in the September 23, 2020 post ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content