This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Jason was very skeptical of STEMI. This also argues against STEMI. Look for old ECGs Do serial ECGs Do echocardiography == MY Comment by K EN G RAUER, MD ( 10/1/2020 ): == From time to time — it's helpful to "resurface" prior cases that convey timeless important lessons. He complained of 3 days of diarrhea and abdominal pain.
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al.
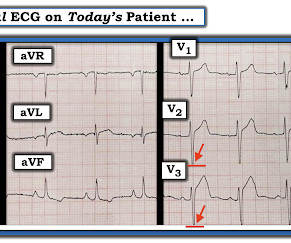
PEARL # 4: As alluded to above — the finding of a Tall R Wave in Lead V1 should prompt consideration of the following LIST of the 6 most common Causes: i ) WPW; ii ) RBBB; iii ) RVH; iv ) Posterior MI; v ) HCM ( Hypertrophic CardioMyopathy ); and , vi ) Normal variant — as a diagnosis of exclusion ( See ECG Blog #81 for more on this issue ).
The cardiologists decided to overrule the STEMI criteria and the cath lab activation was NOT cancelled, and she was taken immediately to the cath lab and found to have an acute thrombotic distal LAD occlusion (TIMI 0). At triage she stated her pain is still persistent, but it is mildly improved compared to when she decided to come to the ED.
For technical reasons — P waves are not well visible in this tracing — BUT — the P wave in lead I appears to be larger than the P wave in lead II , which is often a tip-off to LA-LL Reversal ( See My Comment in the November 19, 2020 and the May 24, 2022 posts in Dr. Smith's ECG Blog ).
Prehospital Conventional algorithm interpretation: ANTERIOR INFARCT, STEMI Transformed ECG by PM Cardio: PM Cardio AI Bot interpretation: OMI with High Confidence What do you think? Example here: DIffuse ST Elevation with Apical Ballooning: is it Takotsubo Stress Cardiomyopathy? She had acute pulmonary edema on exam.
So Shark Fin really is just a dramatic representation of STEMI, and can be in any coronary distribution. So this is STEMI, right? I have summarized the m ajor e tiologic c ategories of acute myocarditis and inflammatory cardiomyopathies. It is often confused with a wide QRS due to conditions such as hyperkalemia. Which artery?
Jason was very skeptical of STEMI. This also argues against STEMI. Look for old ECGs Do serial ECGs Do echocardiography June 17, 2016 Anterior STEMI? He complained of 3 days of diarrhea and abdominal pain. The medics recorded a prehospital ECG: The computerized QTc is 397 ms Jason writes: " What's your thoughts Steve?"
by making it clear to everyone that this is NOT an EKG that one sees with takotsubo cardiomyopathy. Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. From Gue at al.
The medics were worried about STEMI, as it meets STEMI criteria. He was admitted for monitoring, as his risk of a ventricular dysrhythmia as cause of the syncope is high ( very high due to HFrEF and ischemic cardiomyopathy ). The troponins are NOT consistent with STEMI (OMI), which typically has a troponin I of at least 5 ng/mL.
Subsequent testing supported the presumption of apical cardiomyopathy as the cause of this patient's sustained VT. ie, Severe subendocardial ischemia from sustained VT in a patient severe apical cardiomyopathy resulted in a peak troponin >31,000 ng/L in today's case ). CT coronary angiogram showed no obstructive coronary disease.
Smith and Meyers to diagnose both obvious (STEMI) and subtle OMI. Stress induced cardiomyopathy (Takotsubo like LV dysfunction) possible The appearance of wall motion abnormalities in some apical views suggest possibility of stress mediated cardiomyopathy. It was trained by Drs.
From My Comment in the November 15, 2023 post in Dr. Smith's ECG Blog: Clinical Points about MINOCA: Given the literature citing a 5-15% estimated incidence of MINOCA in patients initially diagosed as having a STEMI or "NSTEMI" — it is important to be aware of the more common entities associated with this entity ( See Figure-2 ).
This ECG clearly meets STEMI criteria by the way, regardless of age or gender. As always, Takotsubo stress cardiomyopathy and focal myocarditis are rare possibilities which can only be proven after a negative cath. This is a high troponin (most STEMI are above 10 ng/mL for troponin I). There is no STE or STD in III an aVF.
He had a h/o ischemic cardiomyopathy and right MCA stroke. Dyspnea, Right Bundle Branch block, and ST elevation Here are two more cases where the differential diagnosis is acute OMI vs. LV aneurysm: Is this acute STEMI? Later, I obtained more clinical history. Instead, he complained of left chest "itchiness". LV Aneurysm?
Hypertrophic Cardiomyopathy or Normal ("Variant")? Anterior STEMI? Potential Adverse Cardiovascular Effects From Excessive Endurance Exercise Exercise Is Medicine? The Cardiorespiratory Implications of Ultra-marathon Bjørkavoll‐Bergseth et al. What does this ECG with significant ST Elevation represent? What is it?
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease.
As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. The provider contacted cardiology to discuss the case, but cardiology "didn't think it was a STEMI, didn't think he needed emergent cath." Canto et al.
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. 50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. Covid PCR negative.
They recorded this ECG: Obvious inferior STEMI/OMI What else? The EMS ECGs: As per Dr. Smith the diagnosis of acute inferior STEMI is obvious from the history of new, severe CP in a patient with the initial EMS ECG that I show below ( TOP tracing in Figure-1 ). He called 911. Medics recorded a BP of 79/52 with pulse of 47.
ECG met STEMI criteria and was labeled STEMI by computer interpretation. J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). Take home : Not all STEs are STEMIs or OMIs. What do you think?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content