This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
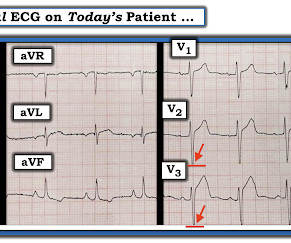
I went to the patient's chart: Elderly woman with stuttering chestpain and SOB, and dizziness. This is a very typical ECG for Hypertrophic Cardiomyopathy. For more on Giant T waves — See My Comment at the bottom of the page in the June 22, 2020 and September 19, 2022 posts in Dr. Smith's ECG Blog ).
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. He has a medical hx notable for hypertension, hyperlipidemia and previous tobacco use disorder.
There were no injuries and no chestpain and he appeared well. He complained of 3 days of diarrhea and abdominal pain. Pretest probability: Especially when there is no Chestpain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear.
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. Stress induced cardiomyopathy (Takotsubo like LV dysfunction) possible The appearance of wall motion abnormalities in some apical views suggest possibility of stress mediated cardiomyopathy. What do you think?
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chestpain and shortness of breath after finishing a 4-mile run. His symptoms of chestpain and shortness of breath were attributed to an asthma exacerbation during exercise.
Takotsubo cardiomyopathy is also a possible explanation. An echo was done and decision was made to pursue cath lab the following day as the echocardiography was interpreted as consistent with Takotsubo Cardiomyopathy. Maybe it is T wave inversion of Takotsubo Cardiomyopathy ? There was never any severe chestpain.
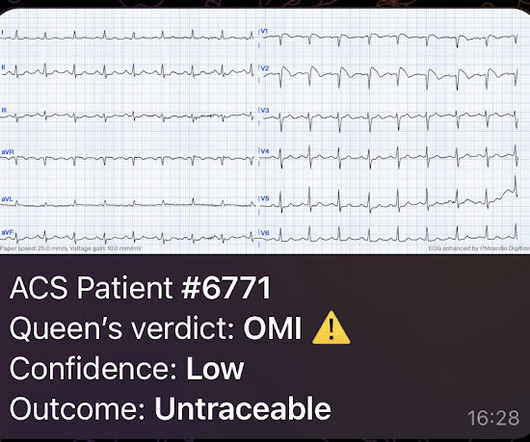
As noticed by the AI, if the patient presented with chestpain , then even this subtle ECG is diagnostic of OMI. Taking a Closer LOOK: We have periodically reviewed cases with low voltage in Dr. Smith’s ECG Blog ( Please see My Comment at the bottom of the page in the November 12, 2020 post, among others ). What do you think?
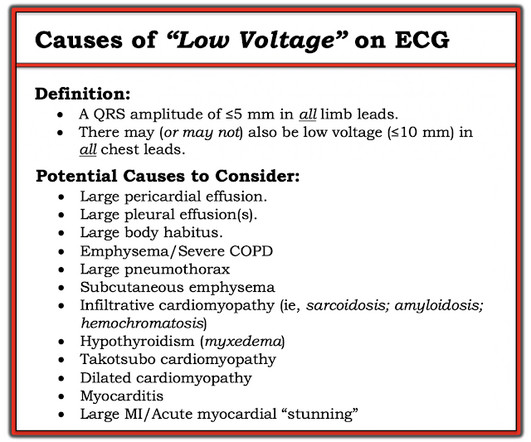
This middle aged patient presented with chestpain: What do you think? As review — I've copied the Table in Figure-2 from previous discussions of potential causes of Low Voltage ( See My Comment in the October 15, 2023 — the November 12, 2020 — and the January 24, 2020 posts in Dr. Smith's ECG Blog ).
There were no injuries and no chestpain and he appeared well. He complained of 3 days of diarrhea and abdominal pain. Pretest probability: Especially when there is no Chestpain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m. 12:15 p.m.
On the other hand — the ST elevation seen in lead V1 is perfectly consistent with LVH and LV "strain" ( ie, The shape of this ST-T wave in lead V1, in association with the deep S wave in this lead — is a mirror-image opposite picture of the typical expected appearance of LVH with "strain" in a lateral chest lead ).
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
The patient's chestpain had resolved by the time of the ECG 2. But it does prove that the patient has coronary disease and makes the probability that his chestpain is due to ACS very very high. He presents with an episode of brief, new-onset chestpain that had resolved by the time E CG # 1 was obtained.
The diagnosis was made based on classic findings of inflammation on an electrocardiogram associated with acute chestpain. 2-3 days after this he developed the same sharp chestpain and shortness of breath with elevated inflammatory markers (CRP) as well as typical findings of pericarditis seen on ECG.
Subsequent testing supported the presumption of apical cardiomyopathy as the cause of this patient's sustained VT. ie, Severe subendocardial ischemia from sustained VT in a patient severe apical cardiomyopathy resulted in a peak troponin >31,000 ng/L in today's case ). CT coronary angiogram showed no obstructive coronary disease.
While fully acknowledging that "Sometimes ya gotta be there!" — in order to optimally assess the patient — the clinical definition of hemodynamic stability is for the patient to be without significant symptoms such as chestpain, shortness of breath, hypotension and/or mental status changes — as a direct result of the fast heart rate.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
He was admitted for monitoring, as his risk of a ventricular dysrhythmia as cause of the syncope is high ( very high due to HFrEF and ischemic cardiomyopathy ). He denied chestpain or dyspnea throughout. The estimated LV ejection fraction is 35%. No previous study for comparison.
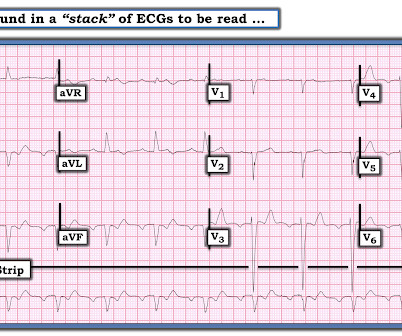
Diagnosis : Extremely slow Atrial flutter == MY Comment , by K EN G RAUER, MD ( 11/15/2020 ): == Some of the most interesting ECG cases I have seen have been picked up “reading through a stack of ECGs” — in the same manner that Dr. Smith picked up today’s case. There was no chestpain — and all troponins were negative.
Instead, he complained of left chest "itchiness". He had a h/o ischemic cardiomyopathy and right MCA stroke. 9 Hours of ChestPain and Deep Q-waves: Is it too late for Thrombolytics? Later, I obtained more clinical history. The patient initially presented with a report of SOB prehospital, but this he denied. LV Aneurysm?
As always, Takotsubo stress cardiomyopathy and focal myocarditis are rare possibilities which can only be proven after a negative cath. More to come. == MY Comment by K EN G RAUER, MD ( 8/8/2020 ): == I LIKE this case by Dr. Meyers — because of the subtle changes seen on serial tracings. What do you think?
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? Figure-2: Causes of Low Voltage on ECG ( Figure reproduced from My Comment at the bottom of the page in the November 12, 2020 post in Dr. Smith's ECG Blog ). What is ELECTRICAL ALTERNANS?
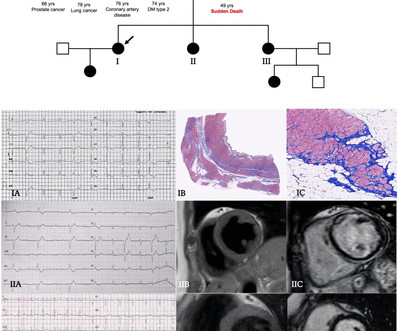
Objectives To describe a cohort of patients with arrhythmogenic left ventricular cardiomyopathy (ALVC), focusing on the spectrum of the clinical presentations. Methods Patients were retrospectively evaluated between January 2012 and June 2020. Of 47 tested patients, 29 (62%) were carriers of a pathogenic/likely pathogenic DNA variant.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. He denied headache or neck pain associated with exertion. Pattern consistent with Takotsubo's cardiomyopathy."
There was no chestpain. The granulomatous inflammation affects the heart, causing an infiltrative cardiomyopathy The most common manifestations of cardiac sarcoidosis are atrioventricular (AV) block and ventricular tachyarrhythmias (VT). This was written by Magnus Nossen The patient is a female in her 50s.
There was some dyspnea but no chestpain. 23/WCC — 2/21/2020 ). 23/WCC — 2/21/2020 ). 23/WCC — 2/21/2020 ). 23/WCC — 2/21/2020 ). A young man presented with continuous prolonged generalized weakness, lightheadedness, and presyncope. Here is his ECG. This shows LVH, with high voltage.
This middle-aged man with no cardiac history but with significant history of methamphetamin and alcohol use presented with chestpain and SOB, worsening over days, with orthopnea. The absence of any wall motion abnormality makes ischemic cardiomyopathy very unlikely. BP:143/99, Pulse 109, Temp 37.2 °C C (99 °F), Resp (!)
Apparently he denied chestpain. As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chestpain.
Smith and Myers found that in otherwise classic Wellens syndrome – that is, prior anginal chestpain that resolves with subsequent dynamic T wave inversions on the ECG – even the T waves of LBBB behave similarly. [2] LBBB is typically the result of preexisting hypertrophy, ischemic heart disease, or cardiomyopathy. 5] Isnard, R.
With OMI, all you know is that your patient has some nonspecific chestpain, SOB, shoulder pain etc. So if the patient is stable, has good LV function on bedside echo, and is relatively young with no history of heart failure or cardiomyopathy, then posterior fascicular VT is likely. which is probably NOT due to acute MI.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content