This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
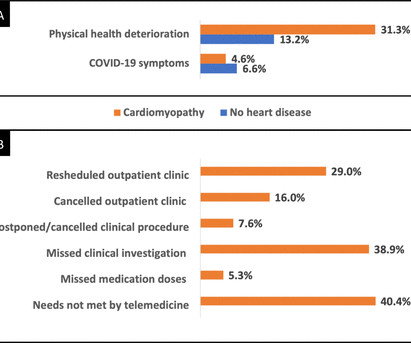
Objectives (1) To evaluate the prevalence and hospitalisation rate of COVID-19 infections among patients with dilated cardiomyopathy (DCM) and hypertrophic cardiomyopathy (HCM) in the Royal Brompton and Harefield Hospital Cardiovascular Research Centre (RBHH CRC) Biobank. (2) of the cardiomyopathy cohort reporting COVID-19 symptoms.
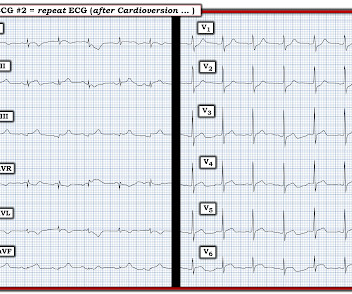
IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ). This left MINOCA as the most likely cause of this patient's symptoms.
Takotsubo cardiomyopathy is also a possible explanation. An echo was done and decision was made to pursue cath lab the following day as the echocardiography was interpreted as consistent with Takotsubo Cardiomyopathy. Maybe it is T wave inversion of Takotsubo Cardiomyopathy ? Are these reperfusion T waves from transient OMI ?
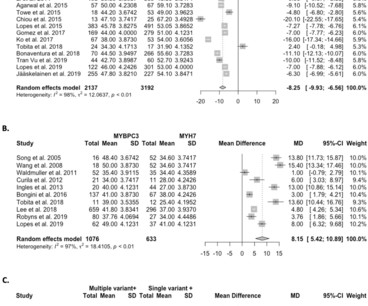
BackgroundIn obstructive hypertrophic cardiomyopathy, myectomy improves symptoms, quality of life, and left ventricular (LV) outflow tract gradients. P=0.24) or Kansas City Cardiomyopathy Questionnaire summary score change (r=0.02,P=0.85), P=0.85), whereas it was significantly associated with change inE/e (r=0.29,P=0.003).ConclusionsIn
Objective This study summarises the diagnostic validity and clinical utility of genetic testing for patients with hypertrophic cardiomyopathy (HCM) and their at-risk relatives. Methods A systematic search was performed in PubMed (MEDLINE), Embase, CINAHL and Cochrane Central Library databases from inception through 2 March 2020.
BACKGROUND:The ability to predict recovery of left ventricular ejection fraction (LVEF) in response to guideline-directed therapy among patients with nonischemic cardiomyopathy is desired. Patients had recent-onset nonischemic cardiomyopathy defined by LVEF 45% and development of symptoms or signs of heart failure within the past 6 months.
Complete left bundle branch block (CLBBB)-like QRS morphology of right ventricular pacing at pacemaker implantation satisfying the American Heart Association/American College of Cardiology Foundation/Heart Rhythm Society criteria of CLBBB was associated with development of pacing induced cardiomyopathy.
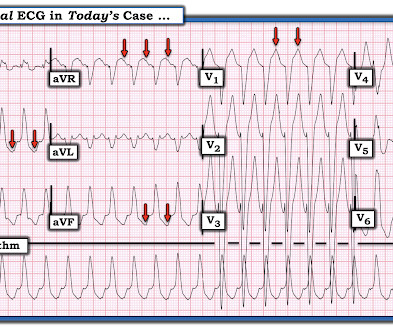
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. The fact that he has a cardiomyopathy argues for a more typical ventricular tachycardia, as does the absence of rSR' in lead V1. It is regular.
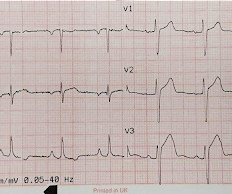
This is a very typical ECG for Hypertrophic Cardiomyopathy. The most recent previous was 4 years prior, and was in the normal range) Elderly patients, and patients with cardiomyopathy (including HOCM), may have troponin values in this range chronically ("chronic myocardial injury").
For technical reasons — P waves are not well visible in this tracing — BUT — the P wave in lead I appears to be larger than the P wave in lead II , which is often a tip-off to LA-LL Reversal ( See My Comment in the November 19, 2020 and the May 24, 2022 posts in Dr. Smith's ECG Blog ).
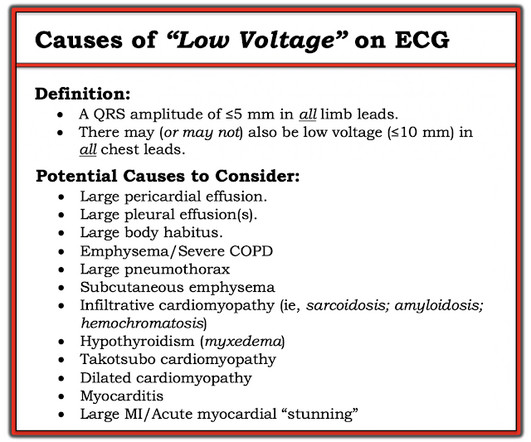
Taking a Closer LOOK: We have periodically reviewed cases with low voltage in Dr. Smith’s ECG Blog ( Please see My Comment at the bottom of the page in the November 12, 2020 post, among others ). 12, 2020 post — are 2 causes potentially relevant to my initial considerations in today’s patient, who was found to have acute LAD OMI.
In simple terms it mimics a heart of Hypertrophic cardiomyopathy, which we know has brisk ejection. We can also understand the principles of the management of cardiomyopathy from a Giraffe’s heart. This forms the basis behind the ventricular reduction and reconstruction surgery for Ischemic dilated cardiomyopathy.(Batisda
Example here: DIffuse ST Elevation with Apical Ballooning: is it Takotsubo Stress Cardiomyopathy? In comparison to the previous study, 11/11/2020, there has been a significant interval deterioration of left ventricular systolic function (previous EF 80%), and there is a new large apical wall motion abnormality.
PEARL # 4: As alluded to above — the finding of a Tall R Wave in Lead V1 should prompt consideration of the following LIST of the 6 most common Causes: i ) WPW; ii ) RBBB; iii ) RVH; iv ) Posterior MI; v ) HCM ( Hypertrophic CardioMyopathy ); and , vi ) Normal variant — as a diagnosis of exclusion ( See ECG Blog #81 for more on this issue ).
The patient was diagnosed with stress cardiomyopathy. Widespread T wave inversions and prolongation of the QT interval is not uncommon in Takotsubo cardiomyopathy. The QTc then gradually shortened over the course of several days as is usual for stress cardiomyopathy. Potassium was 4,8 mmol/l. ( ref 3,5-4,6 mmol/l ).
Recognizing non-sarcomeric Hypertrophic Cardiomyopathy (HCM) by echocardiography is one such task.It With all all these advancements ,how good is echocardiography in ruling out (or in) reversible /treatable HCM mimickers or their molecular subsets. Amyloid -HCM coexistence Medical pathology is never a pure science.It
The most important clinical entity associated with motion alternans is large pericardial effusion — though motion alternans has also been observed in some cases of hypertrophic cardiomyopathy. It is important to appreciate that not all pericardial effusions produce electrical alternans.
In other words, the severely increased end diastolic pressure from the extremely poor LV function caused by the myocarditis results in extremely poor coronary perfusion pressure. == MY Comment by K EN G RAUER, MD ( 2/16/2020 ): == As per the title by Dr. Smith — this case was not what I thought. 109 (20):361-368, 2012 — CLICK HERE ).
Working through a case of a regular WCT Rhythm in this 80-something woman See My Comment in the May 5, 2020 post on Dr. Smiths ECG Blog. Another case of a regular WCT Rhythm in a 60-something woman See My Comment at the bottom of the page in the April 15, 2020 post on Dr. Smiths ECG Blog. Smiths ECG Blog.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m. 12:15 p.m.
Data was obtained from the Hospital Corporation of America (HCA) enterprise-wide database from January 2020 to September 2023 using the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM).
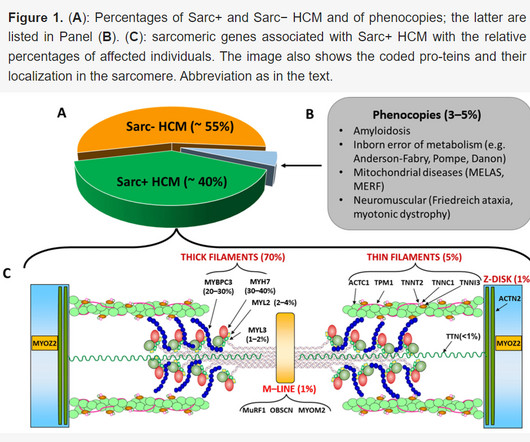
HCM is an "umbrella term" applied to the presence of LVH in the absence of "abnormal cardiac loading conditions" ( Hughes et al — JAHA 9:e015294, 2020 ). . = A bout H CM ( Different Forms of this Entity ): I've excerpted what appears below from My Comment in the December 26, 2023 post in Dr. Smith's ECG Blog.
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. hours T-wave are getting larger again The patient went for an angiogram at about 7 hours after arrival. This is not the case.
Subsequent testing supported the presumption of apical cardiomyopathy as the cause of this patient's sustained VT. ie, Severe subendocardial ischemia from sustained VT in a patient severe apical cardiomyopathy resulted in a peak troponin >31,000 ng/L in today's case ). CT coronary angiogram showed no obstructive coronary disease.
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation.
Stress induced cardiomyopathy (Takotsubo like LV dysfunction) possible The appearance of wall motion abnormalities in some apical views suggest possibility of stress mediated cardiomyopathy. Regional wall motion abnormality-distal septum anterior and apex. Regional wall motion abnormality-distal inferior wall.
As I have discussed the user-friendly and time-efficient criteria I favor for distinction between VT vs SVT rhythms ( with either preexisting BBB or aberrant conduction ) — I'll refer those interested in more detail to My Comments in the May 5, 2020 — the April 2, 2022 — and the February 14, 2022 posts in Dr. Smith's Blog.
Look for old ECGs Do serial ECGs Do echocardiography == MY Comment by K EN G RAUER, MD ( 10/1/2020 ): == From time to time — it's helpful to "resurface" prior cases that convey timeless important lessons. The diagnostic problem posed in today's repost from June 17, 2016 is a perfect example of this.
by making it clear to everyone that this is NOT an EKG that one sees with takotsubo cardiomyopathy. Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy.
Or Benign Early Repolarization? = == MY Comment by K EN G RAUER, MD ( 10/1/2020 — edited on 2/4/2023 — ): == From time to time — it's helpful to "resurface" prior cases that convey timeless important lessons. Look for old ECGs Do serial ECGs Do echocardiography June 17, 2016 Anterior STEMI?
Seen together, these 2 ECG findings suggest possible RVH ( For review on "My Take" for the ECG diagnosis of RVH — Please see My Comment at the bottom of the page in the March 6, 2022 post and in the September 1, 2020 post of Dr. Smith's ECG Blog ). As per Dr. Smith — I was happy to learn that this patient was going to cath!
He was admitted for monitoring, as his risk of a ventricular dysrhythmia as cause of the syncope is high ( very high due to HFrEF and ischemic cardiomyopathy ). IF you missed the KEY Findings on the pre-hospital ECG of todays case Please take another look at My Comment at the bottom of the page of that February 6, 2020 post.
Takotsubo (ie, Stress ) Cardiomyopathy. These cases provide insight to assessment for MAT: The January 5, 2020 post in Dr. Smith’s ECG Blog — for an example of MAT. Myocardial injury with Covid may arise from a number of potential causes — which include: Acute myocarditis. Acute Right Heart Strain. Acute pulmonary embolus.
To paraphrase Dr. Smith's comments in the May 19, 2020 post : — Non-obstructive coronary disease does not ne cessarily imply no plaque rupture with thrombus. This is not the case. There is a trend toward these patients being younger — with a greater relative percentage of women — and fewer traditional cardiac risk factors.
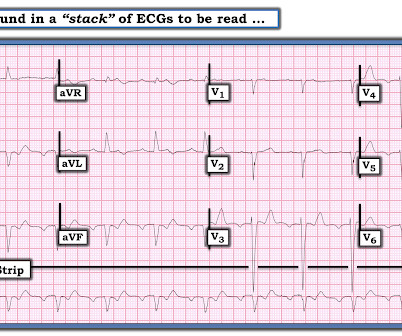
Diagnosis : Extremely slow Atrial flutter == MY Comment , by K EN G RAUER, MD ( 11/15/2020 ): == Some of the most interesting ECG cases I have seen have been picked up “reading through a stack of ECGs” — in the same manner that Dr. Smith picked up today’s case. It turned out that he had a history of slow atrial flutter.
Very good summary of the data on Fractional Flow Reserve and Instantaneous Wave Free Ratio: [link] == MY Comment by K EN G RAUER, MD ( 1/31/2020 ): == Interesting case to review! We are told that this middle-aged male patient has a history of prior MI with stents.
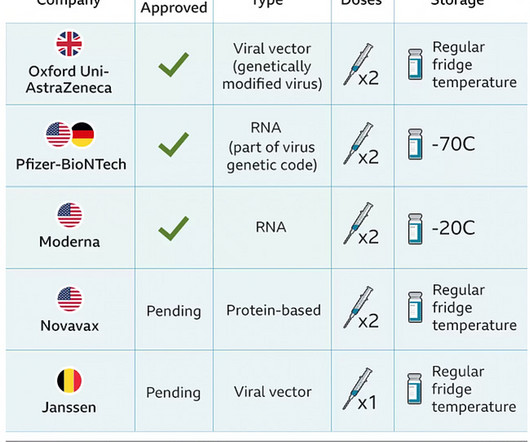
Events of cardiomyopathy or cardiac failure were reported by eight participants after the Novavax COVID-19 Vaccine, Adjuvanted (0.03%) and one participant after placebo (<0.01%). Myocarditis and/or pericarditis were reported by two participants after the Novavax COVID-19 Vaccine, Adjuvanted (0.01%) and no participants after placebo.
He had a h/o ischemic cardiomyopathy and right MCA stroke. For another example of intermittent RBBB conduction, in which a similar initial deflection with terminal delay facilitated recognition of RBBB Conduction — Please SEE the June 25, 2020 post in Dr. Smith's Blog. Later, I obtained more clinical history.
Figure-2: Causes of Low Voltage on ECG ( Figure reproduced from My Comment at the bottom of the page in the November 12, 2020 post in Dr. Smith's ECG Blog ). Figure reproduced from My Comment at the bottom of the page in the September 7, 2020 post in Dr. Smith's ECG Blog ). What is ELECTRICAL ALTERNANS?
Hypertrophic Cardiomyopathy or Normal ("Variant")? Potential Adverse Cardiovascular Effects From Excessive Endurance Exercise Exercise Is Medicine? The Cardiorespiratory Implications of Ultra-marathon Bjørkavoll‐Bergseth et al. Both cTnI and cTnT increased in all individuals, reaching the highest level at 3 hours after the race.
Physicians initially attributed symptoms to “panic, anxiety or stress” in half of these patients, with women more likely than men to have their symptoms attributed to psychiatric causes (65% vs. 32%; P < 04). == MY Comment by K EN G RAUER, MD ( 9/7/2020 ): == Interesting case with thorough discussion by Dr. Smith on arrhythmia management.
As always, Takotsubo stress cardiomyopathy and focal myocarditis are rare possibilities which can only be proven after a negative cath. More to come. == MY Comment by K EN G RAUER, MD ( 8/8/2020 ): == I LIKE this case by Dr. Meyers — because of the subtle changes seen on serial tracings. What do you think?
Objectives To describe a cohort of patients with arrhythmogenic left ventricular cardiomyopathy (ALVC), focusing on the spectrum of the clinical presentations. Methods Patients were retrospectively evaluated between January 2012 and June 2020. Results Fifty-two patients (63% males, age 45 years (31–53)) composed the study cohort.
The mortality rate of alcohol-related cardiomyopathy using ICD code I42.6 Alcoholic cardiomyopathy) was studied from 2001-2020. 100,000 deaths.Conclusions:The mortality trends associated with alcohol-related cardiomyopathy have not changed significantly over the past two decades. 100,000 deaths in four U.S
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content