This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
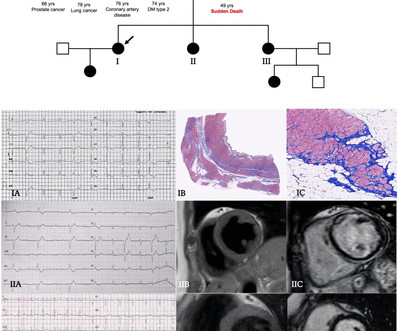
Objectives To describe a cohort of patients with arrhythmogenic left ventricular cardiomyopathy (ALVC), focusing on the spectrum of the clinical presentations. Methods Patients were retrospectively evaluated between January 2012 and June 2020. Results Fifty-two patients (63% males, age 45 years (31–53)) composed the study cohort.
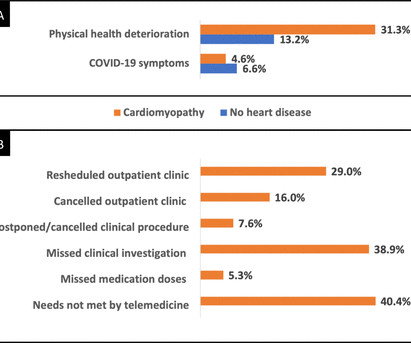
Objectives (1) To evaluate the prevalence and hospitalisation rate of COVID-19 infections among patients with dilated cardiomyopathy (DCM) and hypertrophic cardiomyopathy (HCM) in the Royal Brompton and Harefield Hospital Cardiovascular Research Centre (RBHH CRC) Biobank. (2) of the cardiomyopathy cohort reporting COVID-19 symptoms.
The mortality rate of alcohol-related cardiomyopathy using ICD code I42.6 Alcoholic cardiomyopathy) was studied from 2001-2020. 100,000 deaths.Conclusions:The mortality trends associated with alcohol-related cardiomyopathy have not changed significantly over the past two decades. 100,000 deaths in four U.S
Introduction:Stress Induced Cardiomyopathy is increasingly becoming more prevalent with increasing awareness about disease condition with annual incidence of 30 cases/100000 per year and an incidence of 1-2% in the patients presenting with acute coronary syndrome.[1] for stress induced cardiomyopathy and found 10450 patients in the data base.
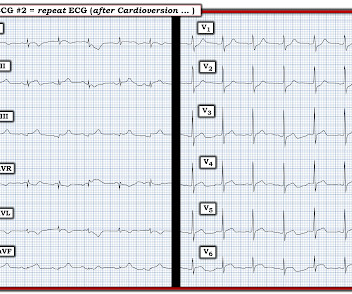
IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ). This left MINOCA as the most likely cause of this patient's symptoms.
Hypertrophic cardiomyopathy (HCM)-related sudden cardiac death (SCD) rates with contemporary management are low; however, high-intensity exercise can induce fatal arrhythmias in HCM patients. Thus, current guidelines recommend avoiding high-intensity exercise in HCM patients at high risk for SCD1,2.
Takotsubo cardiomyopathy is also a possible explanation. An echo was done and decision was made to pursue cath lab the following day as the echocardiography was interpreted as consistent with Takotsubo Cardiomyopathy. Maybe it is T wave inversion of Takotsubo Cardiomyopathy ? Are these reperfusion T waves from transient OMI ?
BackgroundIn obstructive hypertrophic cardiomyopathy, myectomy improves symptoms, quality of life, and left ventricular (LV) outflow tract gradients. P=0.24) or Kansas City Cardiomyopathy Questionnaire summary score change (r=0.02,P=0.85), P=0.85), whereas it was significantly associated with change inE/e (r=0.29,P=0.003).ConclusionsIn
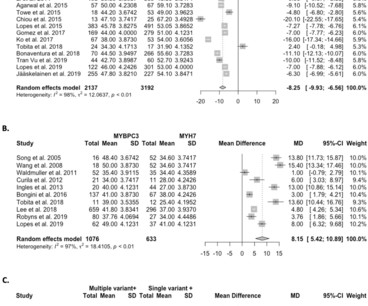
Objective This study summarises the diagnostic validity and clinical utility of genetic testing for patients with hypertrophic cardiomyopathy (HCM) and their at-risk relatives. Methods A systematic search was performed in PubMed (MEDLINE), Embase, CINAHL and Cochrane Central Library databases from inception through 2 March 2020.
While there are several potential reasons for the lack of benefit, an underexplored possible reason is the presence of coincidental non-ischemic cardiomyopathy (NICM). We identified the presence and cause of cardiomyopathy using CMR and coronary angiography data, blinded to clinical outcomes. had no cardiomyopathy (CAD+noCM), 64.8%
BACKGROUND:Over the past decades, hypertrophic cardiomyopathy has become a contemporary treatable disease. There was a significant decline in the rates of sudden cardiac death from 1990 (0.84%/y) to 2020 (0.31%/y).CONCLUSIONS:Dramatic Circulation: Arrhythmia and Electrophysiology, Ahead of Print.
BACKGROUND:The ability to predict recovery of left ventricular ejection fraction (LVEF) in response to guideline-directed therapy among patients with nonischemic cardiomyopathy is desired. Patients had recent-onset nonischemic cardiomyopathy defined by LVEF 45% and development of symptoms or signs of heart failure within the past 6 months.
BackgroundDedicated hypertrophic cardiomyopathy (HCM) center cohorts have reported reductions in HCMrelated deaths, likely due to the introduction of contemporary treatments. Excess HCMrelated deaths were estimated during the 2020 to 2022 COVID19 pandemic. Journal of the American Heart Association, Ahead of Print.
Finally, LV-GLS provided incremental prognostic value over 2020 American College of Cardiology (ACC)/American Heart Association (AHA) risk model (log-likelihood ratios, -262.2 004 for 2020 AHA guideline and 2022 ESC guideline, respectively).Conclusion:Feature to 3.36]) after adjustment for known risk factors. vs -266.2; vs -264.9;
Complete left bundle branch block (CLBBB)-like QRS morphology of right ventricular pacing at pacemaker implantation satisfying the American Heart Association/American College of Cardiology Foundation/Heart Rhythm Society criteria of CLBBB was associated with development of pacing induced cardiomyopathy.
Prior to 2020, studies mapping the electrical activity of the heart had 20 or 30 patients at most. The vest is currently being used to map the hearts of people with diseases such as hypertrophic cardiomyopathy and dilated cardiomyopathy. The vest has since been used successfully in 800 patients.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. The fact that he has a cardiomyopathy argues for a more typical ventricular tachycardia, as does the absence of rSR' in lead V1. It is regular.
This is a very typical ECG for Hypertrophic Cardiomyopathy. The most recent previous was 4 years prior, and was in the normal range) Elderly patients, and patients with cardiomyopathy (including HOCM), may have troponin values in this range chronically ("chronic myocardial injury").
For technical reasons — P waves are not well visible in this tracing — BUT — the P wave in lead I appears to be larger than the P wave in lead II , which is often a tip-off to LA-LL Reversal ( See My Comment in the November 19, 2020 and the May 24, 2022 posts in Dr. Smith's ECG Blog ).
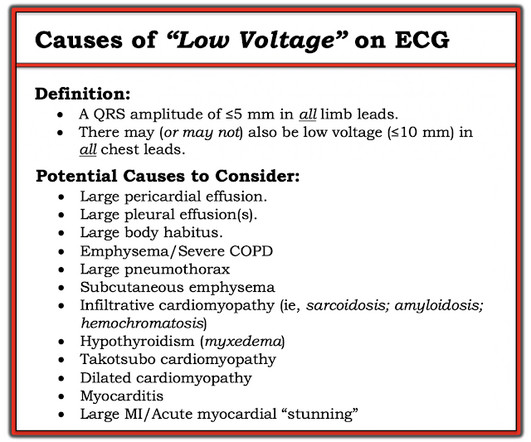
Taking a Closer LOOK: We have periodically reviewed cases with low voltage in Dr. Smith’s ECG Blog ( Please see My Comment at the bottom of the page in the November 12, 2020 post, among others ). 12, 2020 post — are 2 causes potentially relevant to my initial considerations in today’s patient, who was found to have acute LAD OMI.
Candidates listed for rare causes of HF significantly differed in baseline characteristics and had more frequent score exceptions compared with other cardiomyopathies (31.3%, 32.0%, 36.4%, and 16.7% for patients with hypertrophic cardiomyopathy, RCM, congenital heart disease, and other cardiomyopathies). and 0.40, respectively).
In simple terms it mimics a heart of Hypertrophic cardiomyopathy, which we know has brisk ejection. We can also understand the principles of the management of cardiomyopathy from a Giraffe’s heart. This forms the basis behind the ventricular reduction and reconstruction surgery for Ischemic dilated cardiomyopathy.(Batisda
Example here: DIffuse ST Elevation with Apical Ballooning: is it Takotsubo Stress Cardiomyopathy? In comparison to the previous study, 11/11/2020, there has been a significant interval deterioration of left ventricular systolic function (previous EF 80%), and there is a new large apical wall motion abnormality.
PEARL # 4: As alluded to above — the finding of a Tall R Wave in Lead V1 should prompt consideration of the following LIST of the 6 most common Causes: i ) WPW; ii ) RBBB; iii ) RVH; iv ) Posterior MI; v ) HCM ( Hypertrophic CardioMyopathy ); and , vi ) Normal variant — as a diagnosis of exclusion ( See ECG Blog #81 for more on this issue ).
Arrhythmogenic cardiomyopathy Long QT syndrome Hypertrophic cardiomyopathy. That said — in a patient who develops TdP — the overall ECG appearance of this initial ECG is consistent with low K+ and/or low Mg++ ( See My Comment in the May 9, 2020 post — for more on the ECG diagnosis of hypokalemia and hypomagnesemia ).
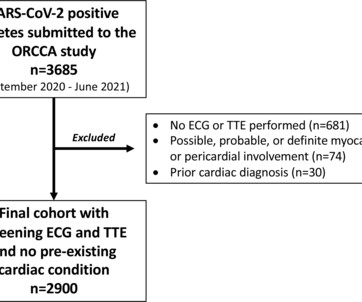
Methods The Outcomes Registry for Cardiac Conditions in Athletes was a nationwide prospective multicentre observational cohort study that captured testing and outcomes data from 45 institutions (September 2020–June 2021). Athletes with an ECG and transthoracic echocardiogram (TTE) and no pre-existing conditions were included.
The patient was diagnosed with stress cardiomyopathy. Widespread T wave inversions and prolongation of the QT interval is not uncommon in Takotsubo cardiomyopathy. The QTc then gradually shortened over the course of several days as is usual for stress cardiomyopathy. Potassium was 4,8 mmol/l. ( ref 3,5-4,6 mmol/l ).
Director of the Hypertrophic Cardiomyopathy Center at the Lahey Hospital and Medical Center. Impact of Aficamten on Disease and Symptom Burden in Obstructive Hypertrophic Cardiomyopathy: Results from SEQUOIA-HCM. CVrg: Heart Failure 2020-2029, p 44; Maron et al. CVrg: Heart Failure 2020-2029, p 44; Maron et al.
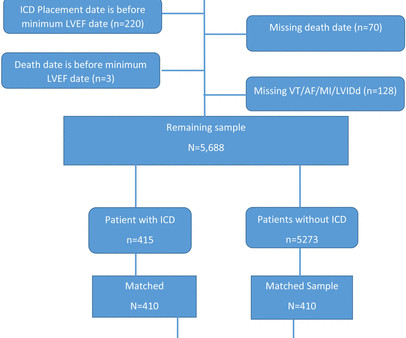
Background Consensus guidelines support the use of implanted cardioverter-defibrillators (ICD) for primary prevention of sudden cardiac death in patients with either non-ischaemic or ischaemic cardiomyopathy with left ventricular ejection fraction (LVEF) ≤35%.
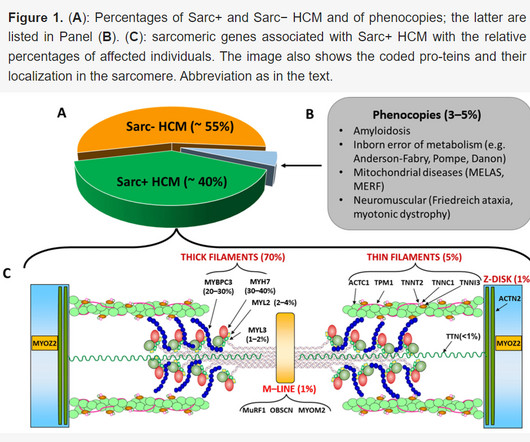
Recognizing non-sarcomeric Hypertrophic Cardiomyopathy (HCM) by echocardiography is one such task.It With all all these advancements ,how good is echocardiography in ruling out (or in) reversible /treatable HCM mimickers or their molecular subsets. Amyloid -HCM coexistence Medical pathology is never a pure science.It
The most important clinical entity associated with motion alternans is large pericardial effusion — though motion alternans has also been observed in some cases of hypertrophic cardiomyopathy. It is important to appreciate that not all pericardial effusions produce electrical alternans.
In other words, the severely increased end diastolic pressure from the extremely poor LV function caused by the myocarditis results in extremely poor coronary perfusion pressure. == MY Comment by K EN G RAUER, MD ( 2/16/2020 ): == As per the title by Dr. Smith — this case was not what I thought. 109 (20):361-368, 2012 — CLICK HERE ).
Working through a case of a regular WCT Rhythm in this 80-something woman See My Comment in the May 5, 2020 post on Dr. Smiths ECG Blog. Another case of a regular WCT Rhythm in a 60-something woman See My Comment at the bottom of the page in the April 15, 2020 post on Dr. Smiths ECG Blog. Smiths ECG Blog.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m. 12:15 p.m.
Data was obtained from the Hospital Corporation of America (HCA) enterprise-wide database from January 2020 to September 2023 using the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM).
The granulomatous inflammation affects the heart, causing an infiltrative cardiomyopathy The most common manifestations of cardiac sarcoidosis are atrioventricular (AV) block and ventricular tachyarrhythmias (VT). Lung involvement is the typical presentation. Cardiac sarcoidosis (CS) is seen in ~10% of patients with sarcoidosis.
See this even more interesting and more dramatic and fascinating case: History of Hypertrophic Cardiomyopathy (HOCM), with Tachycardia and High Lactate = My Comment by K EN G RAUER, MD ( 10/28 /2023 ): = QUESTION: For clarity in Figure-1 — I've reproduced today's ECG without the long lead rhythm strip. 23/WCC — 2/21/2020 ).
HCM is an "umbrella term" applied to the presence of LVH in the absence of "abnormal cardiac loading conditions" ( Hughes et al — JAHA 9:e015294, 2020 ). . = A bout H CM ( Different Forms of this Entity ): I've excerpted what appears below from My Comment in the December 26, 2023 post in Dr. Smith's ECG Blog.
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. hours T-wave are getting larger again The patient went for an angiogram at about 7 hours after arrival. This is not the case.
The World Health Organisation (WHO) formally proclaimed COVID-19, the illness spread by a zoonotic SARS-CoV-2, as a pandemic in March 2020, after it had started to spread in late 2019. Even though the pandemic is on the wane, new studies and evidence about it continue to emerge.
2020) The un-disputable fact is ischemic DCM has a target to treat, though it is termed as cardiomyopathy. Please remember we don’t deny an ICD for a sarcoid cardiomyopathy or end-stage HCM just because they are non-ischemic. Circulation. 2022 Feb 8;145(6):427-436. CRT -P vs CRT-D Samy M, Hamdy RM.
Subsequent testing supported the presumption of apical cardiomyopathy as the cause of this patient's sustained VT. ie, Severe subendocardial ischemia from sustained VT in a patient severe apical cardiomyopathy resulted in a peak troponin >31,000 ng/L in today's case ). CT coronary angiogram showed no obstructive coronary disease.
Brandão M, Desmoplakin Cardiomyopathy: Comprehensive Review of an Increasingly Recognized Entity. The 2020 “Padua Criteria” for Diagnosis and Phenotype Characterization of Arrhythmogenic Cardiomyopathy in Clinical Practice. J Clin Med. J Clin Med. 2022 Jan 5;11(1):279. doi: 10.3390/jcm11010279.
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content