This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Do either, both, or neither have occlusion MI? Vitals were normal.
Bad chest pressure with severe left shoulder pain 3 nights ago. Now appears to be in cardiogenicshock." However, cardiogenicshock usually takes some time to develop, so it is probably subacute." Cardiogenicshock and ACS is an indication for the cath lab, even if you don't think there is OMI.
A 50-something man presented in shock with severe chestpain. The patient was in clinical shock with a lactate of 8. The February 11, 2020 post ( LA-RA reversal ). The March 18, 2020 post ( LA-RA reversal ). The August 28, 2020 post ( LA-LL reversal ). The November 19, 2020 post ( LA-LL reversal ).
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
A middle aged man had off and on chestpain for 2 weeks, then 2 hours of more severe and constant pain. Just prior to transport, the patient became confused and agitated and, although blood pressure and pulse were OK, I was worried about cardiogenicshock. He did not get prehospital activation. What do you think?
He went into cardiogenicshock and is intubated in the cardiac ICU. Cortland : Thank you so much for your reply! I just got the follow up that he had a near complete very proximal LAD occlusion , and a complete PDA occlusion. Not the culprit artery I was expecting but potentially a wraparound LAD?
And some similar ECGs from Pulmonary Embolism: A young woman with altered mental status and hypotension An elderly woman transferred to you for chestpain, shortness of breath, and positive troponin - does she need the cath lab now? Tachycardia is unusual in ACS unless there is cardiogenicshock or a second simultaneous pathology.
This was my response: If it is the right clinical situation, such as acute chest discomfort, it looks like proximal left anterior descending occlusion with right bundle branch block and left anterior fascicular block. Because of the tachcardia, I would expect her to be very poor left ventricular function and maybe Cardiogenicshock.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. What do you think? This is an ominous sign.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Tachycardia is unusual for OMI, unless the patient is in cardiogenicshock (or getting close).
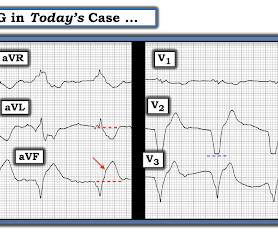
Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiac arrest, cardiogenicshock or impending shock. Here are some cases of RBBB with LAFB: What is the Diagnosis in this 70-something with ChestPain?
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
This pattern is essentially always accompanied by cardiogenicshock and high rates of VT/VF arrest, etc. The patient arrived to the ED in cardiogenicshock but awake. What is the Diagnosis in this 70-something with ChestPain? 68 minutes with chest compressions, full recovery. Eur Heart J.
Written by Pendell Meyers An adult man presented with acute chestpain. See our other cases with similar patters, to burn this deep into your brain files: Smith : In my experience, these cases of LAD OMI with RBBB and LAFB are either about to arrest, post-arrest, and/or in cardiogenicshock. He appeared critically ill.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content