This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
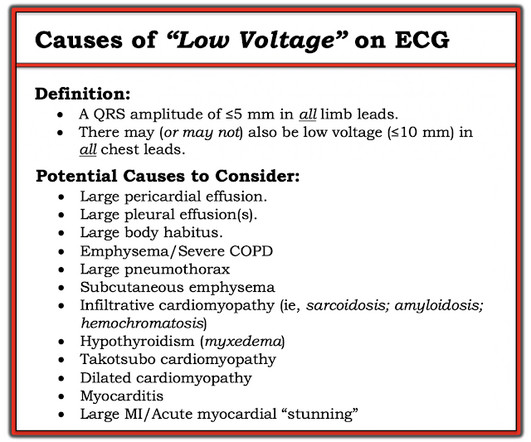
A patient had a cardiacarrest with ventricular fibrillation and was successfully defibrillated. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. These studies did not address OMI ECG findings!!!
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiacarrest. Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. To Emphasize: The phenomenon of T-QRS-D is not needed in today's case to recognize the acute STEMI.
Cardiac Troponin Testing in Patients with COVID-19: A Strategy for Testing and Reporting Results. Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. Guo T, Fan Y, Chen M, et al.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. So, your next step is to Trace it down, and Copy it over".
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS.
For technical reasons — P waves are not well visible in this tracing — BUT — the P wave in lead I appears to be larger than the P wave in lead II , which is often a tip-off to LA-LL Reversal ( See My Comment in the November 19, 2020 and the May 24, 2022 posts in Dr. Smith's ECG Blog ).
Past medical history included RBBB without other cardiac history, but old ECG was not available. The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. As I review in My Comment in the January 16, 2020 post of Dr. Smith's ECG Blog ( and have reproduced in Figure-2 below ) — the ECG of patients with acute LMCA occlusion may be varied. The below ECG was recorded.
She was diagnosed with a Non-STEMI and kept overnight for a next day angiogram. Medics recorded the above ECG and called a STEMI alert. The patient went into arrest pre-hospital. Her symptoms at the time ECG #1 was obtained were CP and SOB — yet interpretation of this initial tracing prompted a STEMI alert.
The provider contacted cardiology to discuss the case, but cardiology "didn't think it was a STEMI, didn't think he needed emergent cath." About two hours after admission, he suffered a cardiacarrest (whether it was VF/VT or PEA is not available) and expired. The whole paradigm is literally called "STEMI" vs. "NSTEMI."
This is a troponin I level that is almost exclusively seen in STEMI. I suspect this is Type 2 MI due to prolonged severe hypotension from cardiacarrest. So this is either a case of MINOCA, or a case of Type II STEMI. If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA.
He has done a lot of great work on cardiacarrest, including as co-author of our study on esmolol in refractory cardiacarrest, and much more with Keith Lurie. This was sent by Guillaume Debaty, from the Grenoble Region of France. See his Google Scholar profile here. Several of these are present in this case.
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiacarrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). The August 22, 2020 post in Dr. Smith's ECG Blog — which illustrates another case of dynamic ST-T wave changes that resulted from a repolarization variant.
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". Hyperkalemia mimics STEMI and OMI in many distributions, but probably the most common is the Brugada morphology in V1-V2 which mimics anterior OMI for those who cannot recognize the Brugada pattern. HyperKalemia with CardiacArrest.
If it is STEMI, it would have to be RBBB with STEMI. This ECG pattern may be diagnostic of B rugada S yndrome IF seen in association with: i ) a history of cardiacarrest; polymorphic VT; or of non-vagal syncope; and / or ii ) a positive family history of sudden death at an early age; and / or iii ) a similar ECG in relatives.
At some point ~1-2 hours after the initial ECG — the patient developed runs of VT, leading to cardiacarrest. This blog post reviews the basics for predicting the " C ulprit" A rtery — as well as the importance of the term, " O MI" ( = O cclusion-based MI ) as an improvement from the outdated STEMI paradigm.
But limitation of this ST elevation to a single lead is not consistent with any distribution of a STEMI. Unfortunately — the patient abruptly developed hypoxemia, followed by cardiacarrest with PEA. It was thought that this action precipitated the patient's desaturation, and led to his cardiacarrest.
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. Then they did an MRI: Patient underwent cardiac MRI on 10/4 that showed mildly reduced BiV systolic function. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al.
This pattern is essentially always accompanied by cardiogenic shock and high rates of VT/VF arrest, etc. Code STEMI was activated. Plus recommendations from a 5-member panel on cardiacarrest. A man in his 80s with chest pain What, besides large anterior STEMI, is so ominous about this ECG? Eur Heart J.
See many examples of Pseudo STEMI due to hyperkalemia at these two posts: Acute respiratory distress: Correct interpretation of the initial and serial ECG findings, with aggressive management, might have saved his life. I've reproduced this figure from My Comment in the January 6, 2020 post of Dr. Smith's ECG Blog ).
This is a case written by Dan Lee (One of our fantastic Hennepin Residents, class of 2020 ) edits by Smith A 60 something-year-old man with a history of ESRD, LVH and prior CABG presented after an episode of hypotension during his hemodialysis, run followed by a syncopal episode which caused his run to be terminated early.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. Bicarb 20, Lactate 4.2,
The computer called this Acute STEMI What do you think? STEMI never has a very short QT. There is Bazett, Fridericia, Hodges, Framingham and Rautaharju -- see here at mdcalc: [link] If the ST Elevation here were due to STEMI, it would be an LAD Occlusion. Treatment is by ICD ( implantable cardioverter defibrillator ).
ECG met STEMI criteria and was labeled STEMI by computer interpretation. J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). Take home : Not all STEs are STEMIs or OMIs. What do you think?
Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!! He was sent back to the waiting room, where he suffered a VF arrest. Approximately 5 minutes after ROSC, this ECG was obtained (about 45 minutes after arrival): Obvious anterolateral OMI, and STEMI criteria positive for those who care or need it.
Acute chest pain, right bundle branch block, no STEMI criteria, and negative initial troponin. Plus recommendations from a 5-member panel on cardiacarrest. Plus recommendations from a 5-member panel on cardiacarrest. These are often VERY difficult to recognized. Protocols can be overridden by Physician Judgment.
2] Curiously, ACLS does not include consideration of calcium in its bradycardia algorithm, which could have prevented the arrest and which along with the epi produced ROSC. HyperKalemia with CardiacArrest. Eur J Emerg Med 2020. regardless of the ECG (when the repeat level came back).[1] References 1. Lindner et al.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content