This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Do either, both, or neither have occlusion MI? Vitals were normal.
Let me tell you about her hospitalization, discharged 1 day prior, but it was at another hospital (I wish I had the ECG from that hospitalization): The patient is 40 years old and presented to another hospital with chestpain and SOB. She had been sitting doing work when she experienced "waves of chest tightness". Sats were 88%.
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. He has a medical hx notable for hypertension, hyperlipidemia and previous tobacco use disorder.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. So, your next step is to Trace it down, and Copy it over".
Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS. Potassium was normal. Cardiology did not think it was "STEMI", but repeated the troponin. Take home 1.
A 60-something woman presented after a witnessed cardiacarrest. This is commonly found after epinephrine for cardiacarrest, but could have been pre-existing and a possible contributing factor to cardiacarrest. A recent similar case: A 40-something with chestpain. Is this inferior MI?
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiacarrest. C ASE C onclusion: As noted above — the middle-aged man in today's case presented to the ED in cardiacarrest. In view of this history — How would YOU interpret the ECG in Figure-1 ?
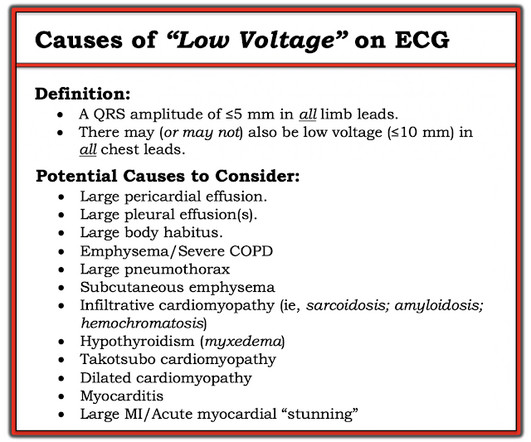
This middle aged patient presented with chestpain: What do you think? As review — I've copied the Table in Figure-2 from previous discussions of potential causes of Low Voltage ( See My Comment in the October 15, 2023 — the November 12, 2020 — and the January 24, 2020 posts in Dr. Smith's ECG Blog ).
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiacarrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). Having looked for negative U waves in patients with chestpain over a period of decades — I'll emphasize that this is not a common finding.
He has done a lot of great work on cardiacarrest, including as co-author of our study on esmolol in refractory cardiacarrest, and much more with Keith Lurie. A 40-something woman was in a remote alpine location when she complained of crushing chestpain. See his Google Scholar profile here.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
Series of Prehospital ECGs Showing Reperfusion == MY Comment by K EN G RAUER, MD ( 9/21/2020 ): == I wish those cardiologists who continue to strictly adhere to STEMI millimeter criteria would begin reading Dr. Smith’s ECG Blog. A mysterious case.
Case submitted by Magnus Nossen MD from Norway, written by Pendell Meyers A man in his 50s with no pertinent medical history suffered a witnessed cardiacarrest. 12 minutes later, the patient went back into VFib arrest and underwent another 15 minutes of resuscitation followed by successful defibrillation and sustained ROSC.
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? Figure-2: Causes of Low Voltage on ECG ( Figure reproduced from My Comment at the bottom of the page in the November 12, 2020 post in Dr. Smith's ECG Blog ). What is ELECTRICAL ALTERNANS?
A patient had a cardiacarrest with ventricular fibrillation and was successfully defibrillated. Coronary Angiography after CardiacArrest without ST-Segment Elevation. N Engl J Med [Internet] 2019;Available from: [link] Should all patients with shockable arrest be taken to angiography regardless of STEMI or No STEMI?
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. What do you think?
The patient presented with chestpain. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. Only 5-18% of ED patients with chestpain have a myocardial infarction of any kind. Is it Brugada pattern?
Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiacarrest, cardiogenic shock or impending shock. Here are some cases of RBBB with LAFB: What is the Diagnosis in this 70-something with ChestPain?
This is a case written by Dan Lee (One of our fantastic Hennepin Residents, class of 2020 ) edits by Smith A 60 something-year-old man with a history of ESRD, LVH and prior CABG presented after an episode of hypotension during his hemodialysis, run followed by a syncopal episode which caused his run to be terminated early. No chestpain.
Other cases of LAD OMI with RBBB/LAFB: A man in his 40s who really needs you to understand his ECG CardiacArrest at the airport, with an easy but important ECG for everyone to recognize A woman in her 60s with 6 hours of chestpain, dyspnea, tachycardia, and hypoxemia Ventricular Fibrillation, ROSC after perfusion restored by ECMO, then ECG.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
Unfortunately — the patient abruptly developed hypoxemia, followed by cardiacarrest with PEA. It was thought that this action precipitated the patient's desaturation, and led to his cardiacarrest. The plan was to proceed as soon as possible with aortic valve replacement. He could not be resuscitated.
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. Steve, what do you think of this ECG in this CardiacArrest Patient?" What is it?
Apparently he denied chestpain. About two hours after admission, he suffered a cardiacarrest (whether it was VF/VT or PEA is not available) and expired. JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chestpain. Here is his first ED ECG: What do you see?
It was from a patient with chestpain: Note the obvious Brugada pattern. The elevated troponin was attributed to either type 2 MI or to non-MI acute myocardial injury. There is no further workup at this time. Smith: Here is a case that was just texted to me today from a former resident. This patient ruled out for MI.
This patient had many complaints including chestpain. Comment by K EN G RAUER, MD ( 2/11 /2023 ): = Today’s case is from a patient with “many complaints”, including chestpain — and, an ECG that raised concern about acute anterior OMI. Chestpain was just one of these complaints. The ioninzed calcium was 6.5
Written by Pendell Meyers A man in his 60s presented with acute chestpain. Smith comment: The patient was lucky to have a cardiacarrest. By undergoing an arrest, providers became aware of his OMI which had not been noticed on his diagnostic ECG, and he thus has a chance at some myocardial salvage.
Written by Pendell Meyers An adult man presented with acute chestpain. Acute chestpain, right bundle branch block, no STEMI criteria, and negative initial troponin. What is the Diagnosis in this 70-something with ChestPain? 68 minutes with chest compressions, full recovery. To quote Drs.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content